
Industry’s Annual Conference
October 15-17, 2026 | Atlanta, GA USA
LEARN
New Here, Start Here →
Understand the Industry…
BUILD
Building or Refining a Practice →
Understand the Mindset & Culture…
Lead
Best Practices. Clear Thinking.
Credible Data. Real-World Insight →
Leadership Hub…
learn the models
Start with foundational knowledge and understand how concierge medicine works.
You’ve got the skills. What you need is A Starting point —
Education, guidance, and tools to help physicians explore concierge medicine with confidence and clarity.


Explore Our resources
Concierge Medicine Today offers a curated portfolio of educational resources developed to support practitioner learning across the concierge medicine continuum. Content is designed to enhance knowledge of concierge practice models, inform operational and strategic decision-making, and strengthen professional leadership competencies. Resources reflect applied expertise and industry-specific insight drawn from the field’s trade publication and annual conference, supporting informed judgment throughout the professional lifecycle.


new released books and industry field Guides

Marketing Your Brand of Membership Medicine (Softcover)
How old-fashioned healthcare delivery methods have been dusted off and rebranded to remind discerning Patients and remarkable Physicians that “It's about being the best Doctor FOR the world.”
“A Doctor’s life moves to a better place when they move at a sustainable pace. I think sometimes there is still skepticism about ‘What is concierge medicine?’ and ‘Hey, what’s the bottom line?’ But I believe we’re starting to see evidence that if Doctor’s don’t do something like this, it will impact the Physician, the Patient, our communities and the bottom line in a negative way. And so that’s one of the things that we’re addressing in this marketing book FOR Doctors. How do you create a remarkable patient experience worth remarking about to others? Hospitality in healthcare, sure, it’s a process but patients today shouldn’t feel processed. Like you, I simply want to leave our healthcare culture in a better place than how it found me and my kids years ago.”
~Editor, Concierge Medicine Today
Pages: 367
Release Date: October 1, 2025
Includes: examples of how some remarkable Doctors practice servant leadership in today’s inconvenient and impersonal healthcare marketplace.
From the Author
"Patients should not be viewed as inconvenient obstacles. Sounds like a compelling opening for a book, doesn’t it? We’ve all encountered dismissive attitudes, rudeness, and negativity within our healthcare system. Despite numerous HR initiatives designed to encourage improvement, many employees resist embracing a more positive mindset towards patients (who are in fact your customer!). This book aims to tackle a pressing issue: why do so many healthcare environments continue to retain these problematic individuals and place them in customer-facing and patient service positions for years and what can we do about it, today? I believe we can do better, and in my view, concierge medicine is leading the way and setting a higher standard. But that’s just my humble opinion."
###
Standard Educational Compliance Notice
Educational resources provided by Concierge Medicine Today are designed to support professional learning and informed decision-making for physicians and practitioners. Content is offered for educational purposes only and does not constitute clinical, legal, or financial advice. Participation in educational activities does not imply endorsement of specific practice models, business arrangements, or outcomes.
Concierge Medicine Today maintains editorial independence and is committed to providing education that is FOR doctors and practitioners—grounded in experience, professional insight, and respect for individual judgment.
Disclosure & Independence
Concierge Medicine Today is an independent trade publication and educational organization. Educational content is developed to provide general information and professional perspective based on industry experience and publicly available sources. Unless otherwise stated, content is not influenced by commercial interests, sponsors, or third parties, and reflects the independent editorial judgment of the authors and contributors.
Educational materials are intended for informational purposes only and should not be construed as legal, financial, or medical advice. Participants are encouraged to evaluate information presented and apply professional judgment appropriate to their individual circumstances.

Improve the Patient Experience (Hardcover Edition)
Like it or not, this is a marketing book, but not in the traditional sense. Old-school marketing tells customers (i.e., patients) that you control the message. Today, that theory doesn’t hold water. Today, new school marketing, especially in healthcare settings, says, “The customers (i.e., patients) inform others about you.”
Embracing concierge medicine, doctors and their medical offices plan for, prepare for, and follow habits in their practice that create a meaningful connection with their patients. This new book by the Editor of the industry’s trade publication, Concierge Medicine Today unpacks the importance of the patient experience highlighting pro tips and spotlighting Physician stories to help you create an irresistible patient experience that leads to more new patient referrals for your concierge medicine or subscription-based healthcare practice.
© 2025 CONCIERGE MEDICINE TODAY, LLC. ALL RIGHTS RESERVED.

All Three Books FOR One Low Price!
Increase Patient Referrals (Softcover)
This all-new book by CMT is your MARKETING + CUSTOMER SERVICE GUIDE that reveals QUICK TIPS on how IMPORTANT CURATING unforgettable experiences ARE FOR PATIENTS!
Pages: 197
Release Date: May 1, 2025
Delivering an exceptional experience for your patients relies on several key elements: location, staff, availability, signage, facilities, and the overall feel of the practice. But let’s be honest, just about every medical office does that and not a lot of patients want to comeback to that environment. Remark-ology refers to how you (and your team!) prepare, greet, inform, and serve each patient who enters your practice. The ultimate aim of remark-ology is to ensure that every interaction leaves patients wanting to return. Healthcare is complicated and it’s filled with unexpected surprises and emotion. Remark-ology wants to help you exceed expectations and turn regretable and forgetable moments into an unforgettable story that patients will remark about to others! This approach not only enhances patient satisfaction but also fosters loyalty and positive word-of-mouth, which are crucial for the long-term success of your ‘remarkable’ practice!

FROM OUR VANTAGE POINT, HOW WE SEE THINGS —
common FAQs
Here’s a quick rundown and a few fast facts and FAQs to get you up to speed on this subscription-driven disruptive shift in our healthcare marketplace.
Are self-pay and cash-only practices categorized within the ‘concierge’ or ‘subscription’ marketplace?
“In summary, the answer is no. This is primarily due to the qualifying term ‘subscription,’” explains the Editor-in-Chief of Concierge Medicine Today. “In the past, sources indicated that there exists an unknown number of independent physicians (or practitioners) working across the U.S. who practice some variation of cash-only or self-pay healthcare, yet are not associated with any marketing label, organization, consulting agency, or brand as we understand them today. While this is likely accurate when examining other facets of the self-pay and cash-pay healthcare landscape, these practitioners technically do not align with the three main subscription-based healthcare delivery models that are predominantly operational in today’s market. Therefore, previous figures estimating these programs in the tens of thousands likely included those self-pay and cash-only practitioners — however, we now observe that the subscription-based healthcare delivery market is robust enough to stand independently and be recognized on its own.”
Are 'concierge' or 'subscription' models in healthcare classified as part of the self-pay and cash-only marketplace?
"In short, yes! However, this is primarily due to the key term 'self-pay,'" remarked the Editor-in-Chief of Concierge Medicine Today. "We're observing an increase in self-pay and cash-only practices within the U.S. healthcare system."
Why the reduced Patient Panels, does this really allow for more focus and attention on the patient?
"Healthcare is a process to be sure, but the patient should never feel processed. More often than not, concierge medicine practices have reduced patient panels of 225-550 to that compared to the traditional, plan reimbursed practices which usually boast 2,500-5,000."
~Editor-in-Chief, Concierge Medicine Today
Is there a strong focus on prevention, routine examinations and a deeper relationship with patients:
"Concierge Medicine practices and programs today are typically known for their focus on prevention and have often curated strong relationships between Patients and the Physician and Patient and the staff. So in essence, staff and Doctors don’t usually have to look at a medical chart to remember your name."
~Editor-in-Chief, Concierge Medicine Today
Are there many self-pay and cash-only healthcare practices in the U.S. today that do not include subscriptions or memberships in their services?
"It's also challenging to pinpoint a specific number," stated the Editor-in-Chief of Concierge Medicine Today. "However, we have observed an increase in the number of self-pay and cash-only healthcare practices across the country. Here's what we've learned over the years about this landscape, which differs from the subscription-based healthcare model: Approximately 13% of family physicians now utilize cash-pay models (American Academy of Family Physicians; 2021); a survey indicates that 43% of practices provide cash payment options (MGMA; 2020); nearly 30% of Americans believe cash payments help reduce costs (Journal of Health Economics; 2022); and specialties like dermatology are increasingly adopting cash-only models due to their simplicity (Health Affairs; 2019)."
first generation
SUBSCRIPTION-BASED HEALTHCARE
According to industry sources from within the bespoke, luxury and ultra-high net worth concierge medicine space, Concierge Medicine Today reports that it is estimated that there are approximately 200-400 doctors across the U.S. and maybe 300-400 abroad.
Bespoke Concierge Medicine Practices (Original Version)
Background: “This is original version of concierge medicine,” says the Editor-in-Chief of the industry’s trade publication, Concierge Medicine Today. “Started by some pioneering and visionary physicians in the 1990’s it’s believed by sources in the industry that while these upscale programs get most of the criticism and commentary, these premium-priced programs present less than 10-15% of the 4,000 subscription-based or membership medicine models operating today. While potentially small in number nationally they do have a nice service offering. While this original and still quite unique form of concierge-style healthcare continues to serve an important purpose and innovate beyond it’s origin story, it is estimated by some close the bespoke subscription practice models that these practices primarily cater to the global citizen, traveler and ultra-high net worth individual and family. It’s estimated that these bespoke concierge medicine models typically charge between $10,000 to $40,000 annually and generally do not market or advertise their services. While media representations of these costly practices often mischaracterize Physicians ambitions for practicing in a business model like this, these stories can often be quite misleading when we all look at how modest and humble most of these doctors are today. I've dedicated my career to illustrating over the past 20 years, that market forces and differing price points exist in healthcare just like in any other marketplace. But it’s important to recognize that luxury service niches exist in every industry, including healthcare, whether your medical school professors like it or not! I’m also of the persuasion that price points for different services and offerings in our economy are perfectly fine. If there’s a market for an ultra-high-end pool table for your basement, go for it. To each there own I say!”
Most Common Myth: Less expensive and more common cash-pay, subscription and membership models with different patient demographics and service offerings often get associated with this high-end version by critics — but more often than not, the criticism is rendered mute given the fact that just like in business, models evolve.
Target Audience: High-Income Earners or individuals with significant disposable income; Executives or busy professionals seeking convenient healthcare access; Wealthy Families or parents looking for comprehensive care for their family; and, Travelers, Global Citizens or people desiring consistent, quality medical care while abroad. (Davis, S., 2019; Health Affairs; "The Rise of Concierge Medicine"; and Lichtenstein, A., 2020; Concierge Medicine Today; "Market Trends in Concierge Healthcare.")
History: For more about the history of bespoke concierge medicine, click here.
most popular, most common
SECOND generation
SUBSCRIPTION-BASED HEALTHCARE
Not to be confused with the bespoke version of concierge medicine, this more modern-version appears to be the most common version of today’s subscription-based, self-pay membership medicine offering.
Personalized Care Models (PCMs) or Today’s More Contemporary Version of Concierge Medicine
PCMs (as we’ll refer to them here for simplicity) have taken a decidedly middle-class and upper middle class practice model (est. 2,000+/- doctors): Today’s most common iteration of modern-day subscription or membership-based healthcare is business model — and like some executive health programs, it remains quietly unconcerned about bespoke or low-cost cash only (i.e. DPC-style) options. These practice models do very little advertising and have patient panels between 200-600 patients and range between $1,500-$2,800 per year. Think of it as the sweet spot in the marketplace. It is also believed that there are around 2,000+/- practices aligned with national enterprises and organizational consultancies that assist Physicians in moving into compliant concierge-style practice models. Today, there are likely 30,000 or more cash healthcare practices in the US.
Business Models Used By Physicians In PCM-style models: Segmented; Hybrid; Full Conversion (SignatureMD; 2025) and click here to learn more and get connected with industry experts and leaders to get started.
Background (More Middle-Class Patients Than Ever): “Although Concierge Medicine started out as a concept for the affluent nearly 20 years ago, over time, the PCM models in the subscription-based and membership medicine space have taken a decidedly middle-class turn and a lot of people don’t recognize that” says the Editor of Concierge Medicine Today, the industry’s healthcare trade publication. “Today, we can see impressions of old-fashioned medical care where a doctor carries a medical bag into your home or visits you when you’re in the hospital because it’s simply the right thing to do. In the past several years, we’ve observed that there are countless people (i.e. prospective patients) searching for these types of doctors every day because their current plan reimbursed, traditional doctor’s office isn’t providing the level of time, attentiveness and relationship they desire from their doctor. The average consumer today no longer equates concierge medicine with only the affluent. From the mid 1990’s to present day, Concierge Medicine has matured into countless less expensive and affordable subscription-based healthcare delivery service variations within our local communities. Annual fees today in most concierge medicine practice environments simply reflect the level of personal attention and service that a doctor provides and noticeably, patients are deciding to make a personal investment in their own healthcare. It’s no longer about being the best Doctor in world, it’s about being the best Doctor FOR the world, FOR your patients and FOR your local community.”
Most Common Myth: “If you were to ask me how most headlines about concierge medicine should accurately read, I would say this: ‘The existence of a wealthy clientele in urban areas prompts a few healthcare practices to develop and promote luxury health services – but there’s also less expensive and very affordable programs and practices out there too!’“ says the Editor of Concierge Medicine Today, the industry’s healthcare trade publication.
Target Audience or Demographics of "Personalized Care Models: Middle and Upper Middle-Class Patients or individuals seeking high-quality, individualized attention; Chronic Disease Patients or those needing tailored management of health conditions; Health-Conscious Individuals or proactive patients looking for customized care; and, Aging Populations and older adults needing specialized care for multiple conditions. (Ralston, R.; 2021; Journal of Personalized Medicine; "Personalized Medicine: A Paradigm Shift in Healthcare."; Zhai, P., & Harris, J.; 2020; American Journal of Managed Care; "The Future of Personalized Healthcare.")
Disruptively Innovative: “No matter how one perceives or understands concierge medicine, along with its subscription and membership options today, most people's first reaction to these novel healthcare delivery concepts is typically curiosity. However, it can also be met with preconceived opinions and criticism,” stated the Editor-in-Chief of Concierge Medicine Today to a gathering of physicians in Atlanta last October. “It's no surprise that much of the criticism directed at these business models comes from a small group of entrenched healthcare professionals who overlook a well-known and essential business principle: ‘disruptive innovation.’ This concept, introduced by Clayton Christensen in the 1990s, explains how smaller companies with limited resources can challenge established businesses by creating new markets or transforming existing ones with simpler, more affordable alternatives. These innovations typically emerge in neglected market segments and gradually ascend, displacing established competitors. Examples include Top Golf revolutionizing the driving range and entertainment sector, Netflix disrupting video rental services, and Uber reshaping the taxi industry — all underscoring the importance of adaptability and innovation for maintaining a competitive edge (Christensen, C. M.; 1997; Christensen, C. M., Horn, M. B., & Johnson, C. W.; 2008; Schindler, R. M., & Pelsmacker, P. De.; 2017; Koller, T., & Wutz, A.; 2018; and Teece, D. J.; 2010). A mentor of mine years ago once shared a thought that has remained with me: ‘Someone is already creating a uniquely better approach, product, environment, or model. There’s someone out there redefining the rules of the current model of whatever it is you do. The aim [he said] isn't necessarily to be the first to create something uniquely better, but rather to be positioned both organizationally and personally to recognize ‘unique’ it when it comes along.’ While I appreciate the altruistic mission of the healthcare field, I observe that much of the criticism aimed at concierge medicine — whether it be the bespoke versions or the more contemporary iterations — originates from within the healthcare system itself. Patients, like myself, generally embrace and appreciate these models. The next generation of patients will require healthcare to innovate as well. While some may dissent ideologically on these models, my experience shows that when the term ‘concierge medicine’ is mentioned, curiosity usually outweighs criticism by both Patients and Physicians. Looking at the bigger picture, I believe we are discouraging more doctors who bring innovative ideas and inadvertently pushing them away when we should be inviting them to the table and expressing interest in their fresh ideas for unique healthcare delivery alternatives. The concept of fairness has not proven effective in healthcare. We must move beyond fairness and actively engage with those waiting on the other side of the exam room or service window today. Ignoring what capable doctors envision for their patient communities benefits no one. The overly complex healthcare marketplace we have today is not truly healthcare; it’s ‘sick care’ and it’s complicated. This ‘sick care’ environment presents numerous reasons for doctors to feel disheartened and potentially leave the medical profession altogether. Concierge medicine (in all of its iterations) has revitalized the careers of many physicians, and to those who argue that it worsens the physician shortage, I would emphasize that five words from my doctor carry immense weight — they are likely one of the most influential voices in my life, second only to my wife and children. It costs little to support a physician's entrepreneurial ideas. When we critique, discourage and fold our arms and stand at the back of the room new ideas in healthcare based solely on fairness regarding shortages, it can come off as simply out of touch and intransigent— so by not listening and failing to encourage innovation in healthcare, we risk losing more physicians to burnout (or worse). Let’s not be in a position where we may overlook the next disruptive innovation, whatever it’s called.”
Growth Expectations
In an article by HealthTech written by Brian Eastwood in December of 2022, Grand View Research estimates that the concierge medicine market will grow more than 10 percent annually each year until 2030. The consultancy cites several factors, including a continued increase in patient volume that started during the pandemic, greater financial stability due to limited reliance on insurance reimbursement, and improved quality of life for physicians. (Eastwood; 2022)
However, the industry’s trade publication, Concierge Medicine Today, has a slightly more conservative estimate of 6-7% growth rate year over year, based on industry observations, physician interviews and experts’ outlook.
Future Forecasts & Trends
According to Precedence Research, a worldwide market research and consulting organization in December of 2023 in a press release (click here) published on Globe Newswire, the U.S. concierge medicine market size accounted for USD 6,633.91 billion in 2023 and grew to USD 6,958.51 million in 2024, expanding at a CAGR of 5.70% between 2023 and 2032. The press release by Precedence Research also said the global concierge medicine market size is projected to surpass USD 34.27 billion by 2032, increasing from USD 19.12 billion in 2023 and is expanding at a CAGR of 6.7% from 2023 to 2032 (Precedence Research; 2023).
STUDIES and DATA SUPPORTING THE PCM or today’s more contemporary concierge medicine and membership MODEL(s)
With the trust gap widening between patients and physicians, it was recently found that 60% of primary care physicians feel they need to earn trust back with patients post-pandemic (MDVIP; 2025) and 1 in 3 reaching “burned out” status – on the Patient Frustration Index, which measures common healthcare pain points across major population groups (MDVIP; 2024). What’s even more remarkable is that around half of these practitioners mentioned have been actively learning from currently successful practices, affiliated organizations and pioneering physicians in the field and experimenting with various subscription and membership pricing models of their own. What’s even more encouraging is that data and studies from the industry reveal some surprising findings:
One study from MDVIP shows personalized primary care reduces ER visits, hospitalizations and outpatient expenditures for diabetic population. The study found that the MDVIP model substantially decreases costs in the diabetic population by year five of enrollment in the preventive care program. After the first post-enrollment year, the mean costs continue to rise for the comparison population, while flattening for MDVIP beneficiaries. The study found decreased unplanned hospital admissions, emergency room visits and outpatient expenditures. At year five, MDVIP patients have statistically significant lower Medicare expenditures. These patients also showed increases in primary care office visits, as their physicians spend more time coaching and monitoring their progress (MDVIP; 2020).
Another study notes that personalized preventive care yields decreased costs and better health management. A study in Population Health Management from MDVIP (MD-Value In Prevention) highlights how a primary care model based on personalized preventive care achieves definitive cost savings and improved health management within three years of adoption. The study, appearing in the February 2016 edition of the peer-reviewed journal, reinforces earlier research published in 2012 in the American Journal of Managed Care (AJMC) proving the efficacy of the MDVIP model(MDVIP; 2016).
And finally, another study proves dramatic reduction in hospitalizations and $300 million savings for MDVIP's Personalized Healthcare Model. MDVIP-affiliated physicians have the time to focus on acute, chronic and preventive health issues, and this increased physician contact time results in improved outcomes for patients and ultimately lowers healthcare costs (MDVIP; 2012, 2013).
How would you some experts define today’s more contemporary version of concierge medicine (present day)? For one last industry perspective, a CEO of one of the conversion companies had this to say to Medical Economics when asked ‘How would you define concierge medicine?’ The CEO said “I would define it simply by saying that physicians elect to reduce their patient panels to much more manageable sizes so they can provide the care their patients deserve. Patients who join the practice pay a membership fee either annually, semiannually or quarterly. In exchange for that membership fee, the patients maintain (or gain) that deep, intimate relationship with their doctor, receive the ability to schedule same-day or next-day appointments and have longer, more comprehensive office visits and annual exams. The practice size typically is reduced from 2,000 to 3,000 patients to 300 to 500. The practice becomes more manageable at that size, and as our affiliated doctors tell us, they have the time to think, plan, dig deeper with their patients and really focus on health, wellness and disease management, not just the symptom of the day. I would [also] say, it’s not for every physician. We receive dozens of inquiries every week from doctors all over the U.S. and engage with between 5% to 8% of them. The ideal candidate is a doctor who’s in internal medicine, family practice or another specialty where there is an ongoing physician-patient relationship. Being located in a market where they’ve been practicing for at least five years is also key. Once they have a following of patients and longer-term relationships, they develop a depth of intimacy with their patients. Also important is that the market where they practice has a median household income above a certain level — and let me add that this is not just for wealthy people. A median household income above $75,000 and median household net worth of $250,000 has proven to be sufficient for patients to make this valuable investment in their health. I don’t want anyone thinking this is only for people in Beverly Hills or New York City. So if it’s the right doctor, in the right market, with the right specialty, today physicians must also have high patient ratings on Google and Healthgrades. Due diligence by both the doctor and the concierge medicine management company must be completed and if everything meets expectations; a detailed plan must be constructed. It takes between 90 and 120 days from the signing of the agreement to the time the concierge practice opens. There are many steps before launch including … ongoing patient communication and engagement, developing a customized website, creating a crystal clear message, confirming a vision for the practice, and training the staff.” (Mazzolini; 2023)
The Industry’s C-Suite Experts Weigh-In Over the Years: For more about the history of personalized care models, click here.
More In-Depth History: For more about the history of personalized care models, click here.
THIRD generation
SUBSCRIPTION-BASED HEALTHCARE
The low-cost version subscription-based healthcare delivery — (not to be confused with Bespoke Concierge Medicine and more contemporary PCM models)
If someone says: “Cash-only DPC is the future”
Our opinion and more correct response isn’t defensive. It’s calm and surgical:
“It may be a future — for some physicians, in some markets, at some stages. But models that survive cycles tend to diversify revenue, integrate with employers, and reduce regulatory exposure. That’s not opinion — that’s pattern recognition.”
~Editor-in-Chief, Concierge Medicine Today
Direct Primary Care (DPC) Models
Often called direct primary care (or DPC): The air space around the DPC model which typically touts it’s no insurance, no Medicare policy is considered to be a low-cost, cash-only healthcare delivery model with a thousand-ish (depending on your sources) around the country. Comprised of a small number of practices but with evangelistic enthusiasm, these Physicians don't want to necessarily have the label 'cheaper' associated with their model but instead prefer the term 'affordable.' While it appears that there are roughly 1,000-1,500+/- cash-only, no insurance, no Medicare, direct primary care (DPC) practices, their fees range in price between $600-$1,200 per year on average, some higher, some lower.
Background, DPC is A DISTANT RELATIVE, BUT NOT CONCIERGE CARE: In the tail end of the 2000s, a spirited group of altruistic doctors (often self-labeling themselves as the “rebels” of healthcare) unveiled something they now call "direct primary care" (DPC). It was once called ‘fee for care’ but that didn’t really stick. It’s been known by a few other names over the years but DPC seems to have stuck; albeit the insider jargon might be a bit clunky from a marketing and advertising perspective it’s a no hassle model (think micro-practice of years ago) attracting new patients and physicians already frustrated with healthcare’s bureaucracy.
How Concierge Medicine and Direct Primary Care Differ:
Direct primary care (DPC) is like concierge medicine in the sense that practices charge a flat fee to patients and offer members greater access to in-person and virtual care. However, there are two key differences. (Eastwood; 2022)
One is that, as the name implies, DPC is solely for primary care, while concierge medicine may also cover specialty care. This tends to make DPC less expensive than concierge medicine but also less comprehensive in the services it can offer. (Eastwood; 2022)
The other is that DPC practices don’t accept insurance, while the American Academy of Private Physicians estimates that 75 percent of concierge medicine practices do. (Generally, concierge practices that don’t accept insurance tend to charge higher membership fees, according to AARP.)
For patients, insurance covers care that’s not included in the membership fee. For practices, insurance reimbursement provides an additional revenue stream; Jorgensen says MDVIP gets about 20 percent of revenue from insurance, which is roughly an even mix of Medicare and commercial plans. (Eastwood; 2022)
Background: Simply put, DPC is a modern-day, cash-only, no insurance, no Medicare, self-pay, reboot or budget-friendly subscription spin on the original 90’s luxury or bespoke concierge medicine subscription model that catered primarily to the affluent clientele years ago. DPC has often been compared and contrasted in the media (and by critics) to its higher priced yet distant relative, bespoke-luxury concierge care and even the PCM models. Conversely, DPC docs often urge their curious colleagues to ditch Medicare and kick insurance headaches to the curb and offer a more affordable fee. They champion a cash-only subscription model for primary care or family health services and those fees can range (typically, but not always) between $55-85/month.
Branding Conundrum: “In contrast, DPC arose as a response to insurance limitations for lower-income populations, focusing on lobbying for legal changes instead of adapting to existing regulations, often leading to violations. Steer clear of marketing and branding, that, while quite prevalent in the marketplace, is frustrating your patient fees achieving qualified medical expense status. For example, you may dearly love the DPC or concierge [as terms or] brands, but, the IRS is convinced that neither brand’s patient fees are qualified medical expenses. Why debate the IRS? Neither brand is likely to fully explain YOUR medical or healthcare philosophy, and neither brand assists with qualified medical expense status so both brands frustrate HSA/FSA/HRA/MSA funding absent changes in tax laws and IRS regulations.” (Eischen; 2025)
Update by Concierge Medicine Today (Jan 1, 2026) — “In light of the new 2025 ‘One Big Beautiful Bill’ Act (effective January 2026), federal law now explicitly allows health savings account (HSA) funds to be used for qualifying direct-primary-care (DPC)/concierge membership fees (Source: dlapiper.com) – but only under specific conditions. Under this law, a fixed-fee DPC arrangement covering only core primary-care services can qualify as a medical expense, provided the monthly membership fee stays under the IRS cap (roughly $150 per individual or $300 per family) (Source: irs.gov). Even so, the core warning remains: simply labeling a practice “concierge” or “DPC” still does not by itself guarantee HSA/FSA/HRA eligibility. Physicians should therefore seek guidance and advice from qualified and competent advisors, communicate carefully and transparently – clearly identifying which membership plans qualify under the new rules and which do not – so patients understand the limits on tax-advantaged payments (Source: dlapiper.comirs.gov).”
Most Common Myth: So while DPC shares some distant genetic traits to other subscription healthcare delivery ancestors, DPC is essentially just a third primary care (or family medicine) subscription healthcare delivery option trying to build its own sand castle on the beach with the some of other subscription options in the healthcare marketplace. Think of DPC as that distant cousin who only pops up at a family reunion every now and then with an interesting take on cash-only, self-pay patients.
Target Audience or Demographics of DPC: Families and Young Adults or individuals seeking transparent and accessible healthcare; Small Business Owners or entrepreneurs wanting straightforward healthcare for employees; Health-Conscious Individuals or patients valuing preventive care; and, Disillusioned Patients or those frustrated with traditional healthcare models. (Tew, J.; 2020; Journal of Health Economics; "Understanding the Demographics of Direct Primary Care."; Peterson, J.; 2021; American Family Physician; "Direct Primary Care: A Review of the Evidence.")
Important Disclaimers, Notes & Professional Considerations:
This page and all content is for educational and reflective purposes only. It is not legal, financial, or medical advice, nor is it a guarantee of success in any practice model. Any transition in business or clinical practice carries risks, complexities, and regulatory considerations. Always consult legal counsel, financial professionals, and experienced advisors before making decisions that impact your practice, patients, or livelihood. Your career is too important—and your calling too valuable—to build on assumption or hurry. Take your time. Seek counsel. And move forward with wisdom and clarity. Some organizations included may also participate as sponsors, exhibitors, or partners in Concierge Medicine Today or Concierge Medicine Forum educational events. Inclusion is based on general industry visibility and does not constitute endorsement or recommendation. Concierge Medicine Today does not receive referral fees or transaction-based compensation from any organization listed. © 2026 Concierge Medicine Today, LLCLEGAL and compliance EXPERTS’ COMMENTARY AND THOUGHTFUL OPERATIONAL CONSIDERATIONS if your considering a concierge medicine or subscription-based healthcare delivery model
Jonna D. Eimer at Roetzel & Andress in Chicago, Illinois.
Jonna D. Eimer is a health law and corporate attorney and shareholder at Roetzel & Andress in Chicago, Illinois. She represents numerous concierge medicine practices and has extensive experience with other innovative practice models. She also advises her clients – including physicians and physician groups, dentists, behavioral health clinicians, and other health care providers – in forming new practices, selling established practices, and negotiating employment and shareholder agreements, as well as guiding them with respect to regulatory matters. In addition, she counsels clients in forming management services organizations (MSOs) and navigating these sales to private equity. Learn More, visit: https://www.ralaw.com/people/jonna-eimer
About Eischen Law Offices
James Eischen, Esq (Jim Eischen) is a licensed California attorney with over 32 years of experience handling complex corporate, business planning, health care and real estate matters. We at Eischen Law Office know that finding the right attorney to represent you is a choice not to be taken lightly. That’s why we offer free consultations to walk you through your needs, the scope of your goals, and your budget. Learn More, visit https://www.eischenlawoffice.com/
About Michele P. Madison
Michele P. Madisone has significant experience in managing legal issues arising in hospitals, physician offices or integrated health systems, including employment, investigations, risk management assessment and corporation management. She provides legal education for health systems’ medical staff, management teams and employees and often facilitates and manages implementation of compliance plans for HIPAA privacy and security regulations. In addition, Michele drafts and completes Certificate of Need applications and facilitates regulatory compliance, and provides oversight and guidance regarding medical staff governance and credentialing issues.
WAXMAN LETTER (circa 2002)
Attached is the March 2002 letter from Congressman Waxman we discussed earlier regarding the Tommy Thompson letter search. Thompson’s reply on behalf of HHS should have followed in March or April 2002. Reading the full exchange, the takeaway is clear: in 2002, HHS essentially signaled that the typical concierge practice model was Medicare compliant.
Source/Credit:
Concierge Medicine Today, LLC. Documents provided from public record via the Tommy G. Thompson Collection, Marquette University Archives. Includes Congressman Waxman’s March 2002 letter and Secretary Tommy G. Thompson’s official response (file noted as “Last Revision”).
Cost Sharing/Expenses
“Another issue confronting concierge practices is cost sharing and how to divide expenses in this type of practice models. Practices must decide if they are allocating costs based on each physician’s patient panel size or based on their respective ownership percentages of the practice. Once you allow for different panel sizes, these differences can become quite problematic, and physicians can end up disagreeing on the fair allocation of these costs. Confronting these differences early in the formation of the practice and providing for them in the practice’s operating documents can help avoid difficult and costly conflicts later for the partners.” (Eimer; 2025)
Medicare/Medicaid/HMO COMPLIANCE
“Collaborate with a knowledgeable attorney, consultant, or individual(s) to structure your cash practice to follow three (3) federal statutes and decades of Medicare/OIG guidance (essentially, using what looks like the executive health model but with different branding and added/variable features). This approach ensures Medicare/Medicaid/HMO compliance, allows for healthcare insurance plan integration (if desired, and not necessary), and ensures patient fees are “qualified medical expenses” eligible for HSA/FSA/HRA/MSA funding (in other words, allows for employer and pre-tax funding) with no changes in existing laws—it works right now.” (Eischen; 2025)
Coverage and Licensing Concerns
“Because of the unique access provided to concierge patients, some practices have added special coverage when these patients are out of state or on vacation. In light of their patients who winter in warmer climates, like Florida, California and Arizona, some practices have partnered with other concierge practices in these states to offer services to their “snowbird” patients. Health systems are taking advantage of these practice models also. For instance, Chicago-based Northwestern Medicine opened a concierge medicine office in Naples, Florida, and Ohio-based Cleveland Clinic also has opened concierge medicine practices in multiple Florida locations. Doctors, however, need to be aware that they need to be licensed in the state where the patient resides. Due to these licensing considerations, some concierge physicians are also obtaining licenses in other states to cover patients that often spend their winters in these warmer states.” (Eimer; 2025)
BE UNIQUE, AVOID INDUSTRY JARGON
“Steer clear of marketing and branding, that, while quite prevalent in the marketplace, is frustrating your patient fees achieving qualified medical expense status. For example, you may dearly love the DPC or concierge [as terms or] brands, but, the IRS is convinced that neither brand’s patient fees are qualified medical expenses. Why debate the IRS? Neither brand is likely to fully explain YOUR medical or healthcare philosophy, and neither brand assists with qualified medical expense status so both brands frustrate HSA/FSA/HRA/MSA funding absent changes in tax laws and IRS regulations.” (Eischen; 2025)
Transitions, Terminations and Retirement
“The concierge model generally relies on increased access and time for patients because physicians have typically accepted fewer patients. Because of this, it can be very difficult to figure out the fairest way to negotiate a partner’s exit and how these patients and fees paid would transfer in the event of such departure. Does the partner get paid only in a buy-out of the whole practice or will the practice buy-out the individual partner upon his or her termination? Would this be handled differently in the case of a retirement? Would the practice consider a buy-out only if another physician can be substituted and take over the patient panel? How then is the new provider paid if fees have already been collected for a given year? It is possible the patients reject the substitute physician regardless of the departing physician’s recommendation.” (Eimer; 2025)
“Oftentimes, the agreements governing the practice’s operations include long notice provisions prior to any termination or retirement because it is not easy to substitute another concierge doctor if one leaves. Also, the patients have paid for the personal relationship and membership with their own doctor, so they do not always feel that this relationship transfers to another doctor. Another thing to consider is if a doctor terminates or unexpectedly dies or becomes disabled and a new doctor cannot cover their patients, what happens to patient fees that have already been collected? The practice needs to consider whether these fees are returned to patients and then whether a new membership agreement is entered into with the new physician. All these considerations need to be addressed in the initial stages of the company’s operations.” (Eimer; 2025)
DON’T ALWAYS FOLLOW THE CROWD
“If your attorney or consultant tells you to opt out of Medicare to do cash healthcare — you are not working with the right expert. Opting out creates different but real compliance risk that the person you are working with does not understand.”(Eischen; 2025)
Don’t replicate, innovate.
“Avoid formulas, brands, and models that work against you implementing your unique vision of healthcare. Don’t replicate, innovate. And, do so using the referenced structuring that for decades has achieved Medicare compliance and tax-advantaged funding options. Call the practice whatever you want, incorporate whatever healthcare services you wish into your subscription, and don’t be constrained by the ill-informed guidance in this marketplace that is not using existing laws/guidance to maximize your practice’s potential.” (Eischen; 2025)
“Because each concierge practice has unique patient fee agreements to consider, there is not a “one size fits all” approach to advising these practices. Concierge practices should not overlook the unique legal and practice issues facing them, from patient fee issues to physician departures. These models have a variety of legal challenges that should be addressed at the early stages of the practice, so they do not lead to partner and patient discord later on.” (Eimer; 2025)
Don’t let Guilt Drive Your Strategy, You’re Worth More Than You Think You Are.
“Instead of allowing a combination of guilt and lack of accurate pricing market data to cause you to under-price and devalue your brand, consider instead pricing your practice at true market value but using ad hoc scholarships/discounts and employer funding to improve equitable access to cash healthcare.” (Eischen; 2025)
Regulatory Considerations
“Concierge practices typically charge a fee for membership in their practice, which generally allows patients increased access to the physicians and their services. If the practice is accepting Medicare and/or commercial insurance, the fee cannot be charged for any service already covered by Medicare or insurance. Additionally, if the practice accepts commercial insurance, the fee must be scrutinized to be sure it is allowed under any agreement with a commercial payor of the practice. Some payor agreements may specifically prohibit any patient fee for membership in a practice. Some practices have reached out to their commercial payors directly when converting to a concierge practice and have had these commercial payors review and approve their patient agreements and membership fees.” (Eimer; 2025)
When you have a heart for your community, you don’t have to compete on price.
“Consider your practice pricing as establishing your perceived brand value in the marketplace. You need not track the national franchise-style concierge enterprise pricing or DPC pricing: both are frequently published, but, most cash practices do not market their prices—so the actual market is much higher than your online search reveals. So the easiest prices to find are not necessarily reflective of the actual market, and imitating them will devalue your perceived brand. Instead, work with an experienced attorney or consultant who actually knows the unpublished typical prices for cash practice models. And remember, most if not all of those published price versions of cash healthcare are not structuring their fees/services to allow for employer/tax-advantaged funding, and perhaps their lower prices are unintentionally reflecting that. Pre-tax and employer funding options allow for higher prices points, and can be used to provide versions of this care with 100% employer funding—that can enable more folks to benefit from this care model.” (Eischen; 2025)
Sales to Third Parties
“Physician owners in a concierge practice also need to consider at the formation of a practice how the profits of the practice will be divided in the case of a sale to a third party. Will profits be divided based on a physician’s ownership in the practice or based on an individual physician’s production and fee generation? If a practice has providers with vastly different production and patient panel sizes, then this is important to consider because the higher producing partner may want a sale to a third party to take into account these differences. Another partner may feel strongly that profits should be divided based on ownership percentages in the practice entity, which may be equal even if the providers have different numbers of patients. Frequently, the potential buyer has their own considerations for valuing the practices and may ascribe different values to each physician’s practice. The buyer may base its valuation of the practice on patient panel size and fees generated by each individual physician.” (Eimer; 2025)
you have options without creating compliance risks.
“If your attorney or consultant tells you that you cannot bill insurance or stay in network while doing cash heallthcare— you are not working with the right expert. There is a wide range of preference with plan billing in cash healthcare. The right expert can explain to you that you can elect to bill plans a little, a lot, or not at all, and why you have those options without creating compliance risks. You can do zero plan billing, or some, but you should know why you have those options, and why there is no need to opt out of Medicare.” (Eischen; 2025)
Industry Reference GUIDES | SELF-HELP SECTION
-

READINESS 101
(PDF Download)
A self-assessment designed to help clinicians evaluate readiness, clarify purpose, and identify next steps before moving into concierge medicine.
-
Foundations 102
(Hardcover Edition)
A beginner’s guide to the business, mindset, and core principles that anchor a successful concierge medicine practice.
-

Marketing 201
(Hardcover Edition)
A strategic playbook for growing your practice through authentic marketing, clear messaging, and relationship-centered systems.
-

Experience 202
(Hardcover Edition)
A guide to crafting a patient experience that is intentional, memorable, and worthy of the concierge medicine standard.
-

Referrals 301
(Softcover Edition)
A framework for building a culture of gratitude, referrals, and repeatable moments that make patients feel known and valued.
-

exit 401
(PDF Download)
A structured, FOR-Doctors assessment that helps you plan a thoughtful, well-timed exit from your concierge medicine practice.

in 2024, according to Concierge Medicine Today, LLC., polling among 300 Concierge Medicine Physician readers at its online trade publication, a listing of the top six areas practicing within the business model from 2014-2024 whom indicated they currently practice within a Concierge Medicine model do so in the following specialties: Family Medicine = 38%; Internal Medicine = 32%; Osteopathic Physician = 9%; Cardiology = 8%; Nephrology = 3%; and Pediatric = 3%
SPECIALTY CONCIERGE MEDICINE FAQs
*
SPECIALTY CONCIERGE MEDICINE FAQs *
Q: To what extent is concierge practice making inroads into specialties?
“Ten years ago, concierge medicine was mostly a primary care adaption story. Today, cardiologists, endocrinologists, OB-GYNs, gastroenterologists, and even oncologists are adopting a compliant business model. And, it’s actually no longer just a practice model—it’s becoming a mindset across medicine. We've observed over the years that concierge medicine physicians have found a more sustainable pace in their practice model whereby they see more clearly that excellence, regardless of it's form, in healthcare, it isn’t just learned and applied clinical skill; it’s also about dignity, attention, timeliness, and clear communication with patients and team members—those aren’t extras, they’re expectations every patient has today. That’s why concierge medicine from our seat on the bus is becoming the new reference point. It’s also why concierge medicine has quickly become from our vantage point the standard others working in healthcare are measured against. The future belongs to physician whom are leaders and whom remove every unnecessary obstacle for the patient and build systems that make servanthood and gratitude for the patient in healthcare repeatable.”
Q: What’s the prevalence of concierge medicine in the U.S.?
A: “Concierge medicine may be small in size, but it’s big on purpose,” notes the industry’s trade publication Editor-in-Chief at Concierge Medicine Today. “While industry sources note year after year that fewer than 2% of all licensed U.S. doctors practice in some version of subscription-based healthcare delivery model—(that’s about 8,000 to 12,000 practices in the U.S.— at least a quarter of those are now specialists. We’ve also observed incremental growth in adoption and entry into these models and it’s been steady at what we hear is about 4–7% a year — some would say higher but we like to stay realistic, not evangelistic. So while concierge medicine is still a small percentage of the 1.1 million U.S. physicians, it’s quickly becoming the new reference point—the model others are measured against.”
Q: Step-by-Step Reality MATH Check 📊
KFF (as of Sept. 2025):
1,105,148 professionally active physicians in the U.S.
(Source: Sept 2025, KFF State Health Policy Data)2% of that total = ~22,100 physicians.
(As noted above) Concierge Medicine Today notes 8,000–12,000 concierge practices.
If each practice averages 1.2 to 1.5 physicians, that translates to roughly 9,600–18,000 concierge physicians, which is well within the “fewer than 2%” range (≈0.9%–1.6% of all U.S. doctors).
So in summary and mathematically speaker, yes — the above statement(s) we believe are mathematically sound and aligns with KFF’s national Professionally Active Physicians and active state licensed physicians from Redi-Data, Inc, September 2025 and our industry sources perpesctive(s).
In short: 📊 Practices ≠ Physicians — and we (CMT) intentionally stay on the conservative side to keep our reporting realistic, not evangelistic — and aim to provide credible estimates.
Q: What are the most common questions physicians ask about moving into concierge practice?
“The three biggest questions physicians ask us are: Can this work for me? How do I tell my patients? What happens to my workload? Underneath each one is a deeper question: Am I being the best doctor I can be for my patients? We then usually encourage them by saying 'It's no longer about being the best Doctor, Specialist, Nurse, Practice Administrator, etc., in the world anymore, it's about being the best Doctor for the world, for your patients and for your local community.'”
Q: Which career stages are most suitable?
“We’ve seen concierge medicine succeed in every career stage—early-career doctors building a foundation is usually the toughest but it has worked for some, mid-career physicians who want to reclaim balance and go deeper into specific conditions with their patients, and late-career doctors choosing to finish well, find a sustainable pace and yet still want to dive deeper into healthcare's more complex questions with their patients. One concierge medicine physician said to me years ago, 'I still work long hours and into the night, I just use my time differently now and I'm a lot happier ... and so are my patients, team and family members.”
Q: What makes it different?
A: “What separates this space isn’t the business model — it’s the mission. It’s the decision to remove unnecessary friction FOR patients and to design systems that make consistency, service, and trust repeatable. Healthcare has always required clinical skill, but from the patient’s perspective, excellence now means dignity, attention, access, and clear communication. Those aren’t luxuries anymore — they’re baseline expectations. That’s why concierge medicine is becoming a reference point. Not because it’s exclusive, but because it’s intentional. Smaller patient panels — hundreds instead of thousands — create room for relationships instead of transactions. And when a model consistently produces better experiences for both patients and physicians, that’s not a trend. That’s a structural shift in how care is being delivered.”
Q: How does the concierge model affect the doctor–patient relationship?
A: “Fewer patients doesn’t mean less care; it means more intentional care, longer careers, and patients who finally feel seen,” adds Concierge Medicine Today’s Editor. “Over the years, when we’ve asked experienced concierge physicians what’s changed for them, they don’t talk about revenue or time off — they talk about joy. These doctors are rediscovering why they started, again. And as one concierge medicine physician reminded us just last month at our industry conference, ‘When the doctor’s fulfilled, the patient benefits too. You can’t fake that kind of energy in an exam room.’ These models are raising the bar for satisfaction on both sides of the room — doctors are staying in practice longer, and patients are reminded what it feels like to be genuinely cared for.”
Q: Which specialties are an ideal fit, and why?
“The specialties that fit best aren’t defined by procedures, but by relationships. Anywhere patients need time, clarity, and ongoing management—cardiology, women’s health, pediatrics, oncology—concierge medicine works. The specialties entering concierge medicine now represent a good percentage of the practices out there today — it's hard to say exactly how many because this is a business model but we're seeing more and more specialties enter this space especially within the past decade and that's encouraging for patients and for Doctors and other healthcare practitioners.”
Q: How much time should physicians plan to prepare, and what are the early steps?
“The average runway I'd estimate is 12–18 months. The first steps aren’t about contracts or spreadsheets—they’re about finding clarity: know your why, talk with your family, surround yourself with a trusted business advisory and consulting team, and learn from a few respected colleagues who’ve made the switch but have humility and are not evangelistic about any particular model of practice. We often encourage Doctors to please do their homework, write down all of their detailed questions and go find the answers with the experts who can put your mind at rest. We often repeat something we read a couple of years ago in a business book that practitoners considering this space find encouraging: ''This learning curve and transitional process won't be easy, but you didn't sign up for easy, you signed up for worthwhile.'”
Q: Are there personality traits that make for successful concierge physicians?
“The physicians who thrive in concierge medicine share four traits: curiosity about patients, humility as leaders, gratitude for those they serve, and a heart for their community. At the end of the day, healthcare isn’t just about medicine—it’s about people. Patients may forget the procedure, the paperwork or what the doctor actually said earlier that day in the exam room, but they’ll never forget how you made them feel.”
Q: Is CONCIERGE MEDICINE EXACERBATING THE PHYSICIAN SHORTAGE?
“Concierge medicine isn’t exacerbating the physician shortage — it’s revealing it,” says Concierge Medicine Today’s Editor-in-Chief. “And that’s a good thing. Every industry eventually faces a moment when disruption forces reflection and reinvention — this is healthcare’s moment. One longtime doctor told us, ‘The system didn’t break overnight. It’s been eroding for decades. Concierge medicine just held up a mirror.’ Critics may not like that, but that’s often what happens when new ideas challenge old assumptions. Change makes people uncomfortable — especially when it highlights what’s not working.”
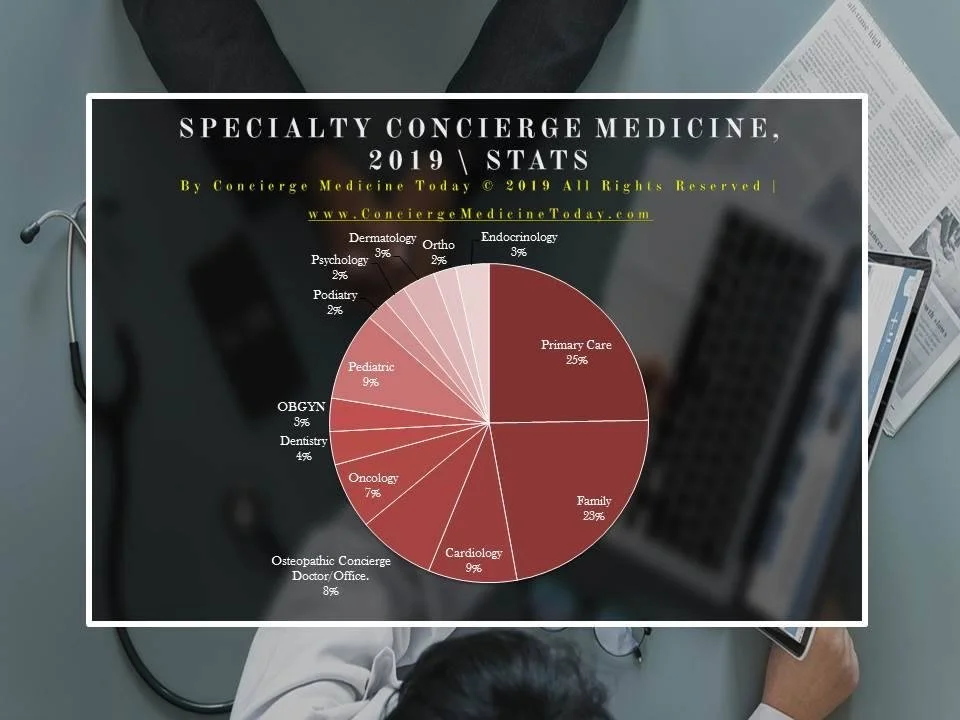
It should be noted as well to the description above that specialist entry into Concierge Medicine is becoming more and more popular[1]. As traditional, plan reimbursed practices continue to see patients in growing numbers that treat symptoms verses focus on preventative aspects of an individual ... and insurance premiums continue to increase, patient interest and their subsequent participation will continue to rise in specialty Concierge Medicine Physician practices in the years ahead. Concierge Medicine Today’s industry sources[1] report that specialty participation by both Physicians and Patients will only continue to increase year over year as more and more chronic conditions require a specialized Physician to quarterback their Patients conditions.
Some specialties not listed above but also indicate they to have a concierge medicine program include, but are not limited to (in no particular order): Integrative Medicine; Pulmonology; Hospital-based programs; Heart and Vascular; Geriatrics; OBGYN; Endocrinology; Doctor of Nursing; Diabetes Specialists’; Dental; Anti-Aging; and more.[2, 3, 4, 5]
Citations and Sources, Credits and Mentions
October 19-21, 2023; Atlanta, GA USA; Concierge Medicine Forum, annual industry conference.
Doctor of Nursing Practice from Raleigh Medical Group is the Latest Provider to Offer Patients the Hybrid Choice™ Concierge Program by Concierge Choice Physicians; NEWS PROVIDED BY Concierge Choice Physicians; 05 Dec, 2023, 08:00 ET; https://www.prnewswire.com/news-releases/doctor-of-nursing-practice-from-raleigh-medical-group-is-the-latest-provider-to-offer-patients-the-hybrid-choice-concierge-program-by-concierge-choice-physicians-302005442.html
Dallas Endocrinologist now offers the Hybrid Choice™ Concierge Program from Concierge Choice Physicians; NEWS PROVIDED BY CONCIERGE CHOICE PHYSICIANS; 03 Mar, 2023, 13:00 ET; https://www.prnewswire.com/news-releases/dallas-endocrinologist-now-offers-the-hybrid-choice-concierge-program-from-concierge-choice-physicians-301762283.html
Integrative Medicine Specialist in Plainfield, IL now offers the latest in patient support and service through the Hybrid Choice™ Program from Concierge Choice Physicians; NEWS PROVIDED BY Concierge Choice Physicians; 21 Jan, 2022, 13:30 ET; https://www.prnewswire.com/news-releases/integrative-medicine-specialist-in-plainfield-il-now-offers-the-latest-in-patient-support-and-service-through-the-hybrid-choice-program-from-concierge-choice-physicians-301465812.html
Dallas/Plano Endocrinologist and Diabetes Specialist now offers patients the Hybrid Choice™ Concierge Program from Concierge Choice Physicians; NEWS PROVIDED BY CONCIERGE CHOICE PHYSICIANS; 26 Oct, 2021, 09:30 ET; https://www.prnewswire.com/news-releases/dallasplano-endocrinologist-and-diabetes-specialist-now-offers-patients-the-hybrid-choice-concierge-program-from-concierge-choice-physicians-301407663.html