BROWSE OUR marketing and PRACTICE growth INSIGHTS
Providing a remarkable experience for your patients depends on a number of strategic marketing factors: staff, culture, vision-casting, signage, facility improvement, interior design, and the overall “feel” of the practice.
ANNUAL CONFERENCE | BASICS | HISTORY AND TIMELINES | ANNUAL REPORT | NATIONAL STATS | TRENDS, POLLS AND SURVEYS | FOR THE MEDIA | SHOP
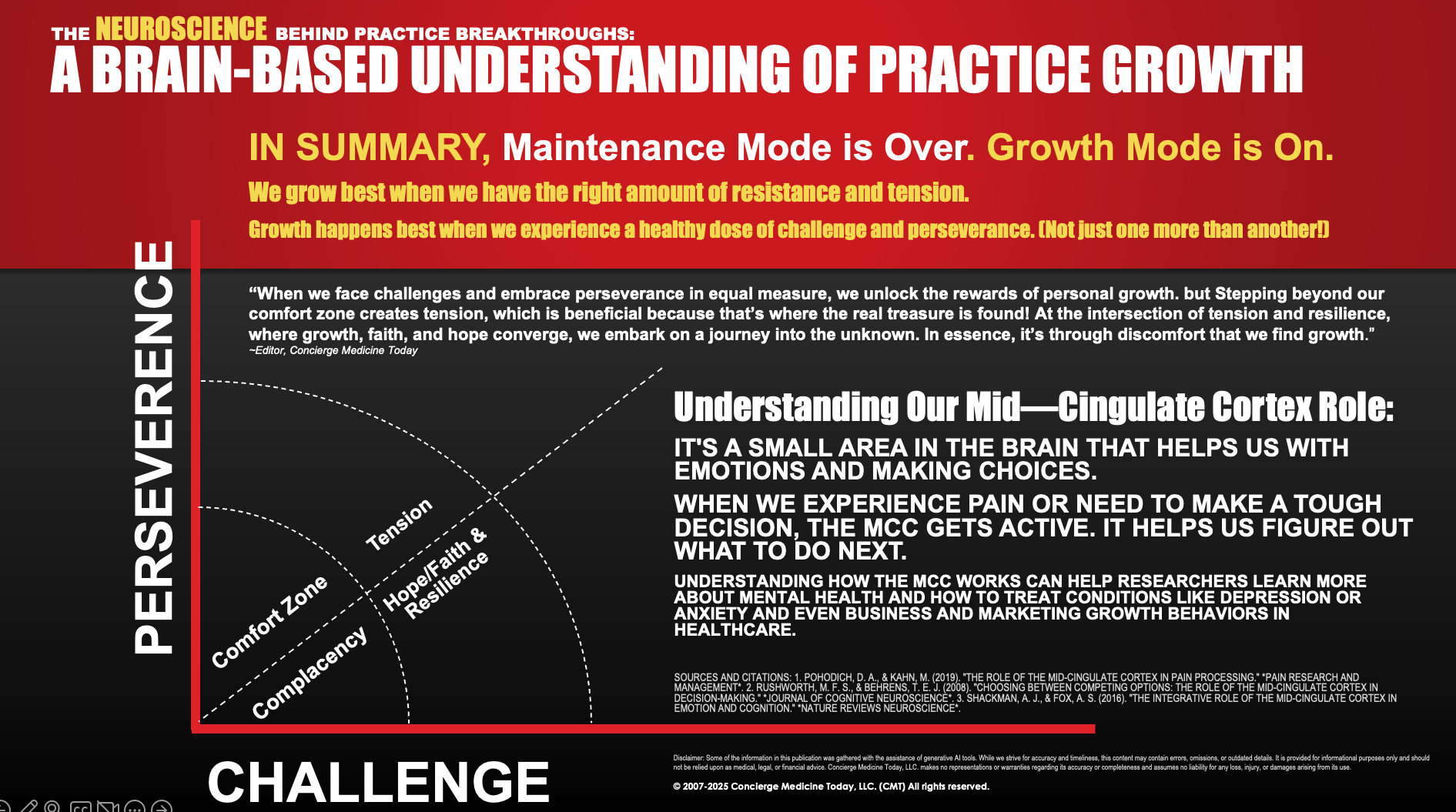



















The neuroscience FRAMEWORK Behind marketing and Practice growth Breakthroughs:
A Brain-Based Understanding of Practice Growth and Marketing.
“When we face challenges and embrace perseverance in equal measure, we unlock the rewards of personal growth. but Stepping beyond our comfort zone creates tension, which is beneficial because that’s where the real treasure is found! At the intersection of tension and resilience, where growth, faith, and hope converge, we embark on a journey into the unknown. In essence, it’s through discomfort that we find growth.”
— Author, Remark-ology
Sources and Citations: 1. Pohodich, D. A., & Kahn, M. (2019). "The role of the mid-cingulate cortex in pain processing." *Pain Research and Management*. 2. Rushworth, M. F. S., & Behrens, T. E. J. (2008). "Choosing between competing options: The role of the mid-cingulate cortex in decision-making." *Journal of Cognitive Neuroscience*. 3. Shackman, A. J., & Fox, A. S. (2016). "The integrative role of the mid-cingulate cortex in emotion and cognition." *Nature Reviews Neuroscience*.

Marketing Reference Guides
-
101: The Basics for Beginners
(Hardcover Edition)
Perfect for newcomers wanting to understand different business models, explore options, and adopt a physician entrepreneur mindset in a competitive economy.
-

201: Marketing Edu. “I just need to grow!” (Hardcover Edition)
(Hardcover Edition, Release Date 10/1/25)
(Now Accepting Preorders)
You've been cozying up to the old-school marketing playbook to grow your practice. But now, it's time to flip the script! Let's pivot from self-promotion to putting your patients front and center.
-

301: Advanced Customer Service Lessons
(Hardcover Edition)
“Time to level up your practice! This isn't a book about how to make your practice bigger. This is a book about how to make your practice more appealing to the people who don’t usually—or have never—gone to practice.”
-

401: Mastering New Patient Referrals by Curating Remarkable Patient Experiences
(Softcover Edition)
For seasoned concierge practices seeking to elevate their patient experience and boost word-of-mouth referrals from existing patients!
The Neuroscience Behind Practice Growth and
Marketing Breakthroughs:
A Brain-Based understanding of Practice Growth
Nominations for Top Physician Leaders in Concierge Medicine
The program encompasses three categories honoring the leadership and achievements of twenty-five individual Physicians in Concierge Medicine to be announced in mid-2025.
FOR IMMEDIATE RELEASE, ATLANTA, GA USA – Nominations are presently being accepted for Concierge Medicine Today’s Top Physician Leaders in Concierge Medicine [of 2025-2026] recognition program, which celebrates the integral role leadership plays in concierge medicine.
“Physicians have been instrumental in driving progress forward in various areas of our healthcare culture,” says the Editor-in-Chief of Concierge Medicine Today. “In modern times, the presence and recognition of Physicians in leadership roles have significantly increased across many specialties, including academics, leading new business endeavors, involvement in hospital leadership, leading advancements in healthcare technology, creating entrepreneurial opportunities for younger medical professionals, leading the conversation about unique healthcare delivery models such as concierge medicine, preventative, diagnostic discussion, A.I., and more.”
Physicians will be recognized by the industry’s trade publication, Concierge Medicine Today, for their answers, perspectives and leadership among the following three criteria:
The Practice of Self-Leadership. Self-leadership involves understanding oneself, managing emotions and behaviors, setting goals, making decisions, and being proactive, self-disciplined, and adaptable.
The Practice of Risk Taking. Risk-taking involves making decisions or engaging in activities with uncertain outcomes. It is essential for personal and professional growth.
The Practice of Delegation. Delegation empowers leaders to entrust tasks and responsibilities to others, harnessing their teams’ diverse skills and talents for greater productivity.
“Often, we take leadership in healthcare for granted and presume that it requires an MBA, a prestigious education, a lofty title, or is strictly reserved only for those with unlimited resources and time to pontificate,” notes the Editor. “Great Physician leaders, particularly in concierge medicine, recognize that there are areas in our healthcare culture where medical practices are unnecessarily giving up influence with patients. Yet, despite the rigors of the marketplace they communicate in such a way that they leverage their strengths for others, provide dignity to everyone around them all the while building productive organizational teams and businesses. Our responsibility as the trade publication isn’t to convince anyone that viewpoints on things like the importance of the Patient-Physician relationship are still paramount or to persuade someone that concierge medicine isn’t what they’ve read about on a blog. Our responsibility is to educate, inform, and, from time to time, showcase the people who organizationally and professionally recognized different when it came along and let you decide how you feel about all of it. We’re here to illuminate, educate, and tip our hats to those who redefine excellence in leadership, specifically those in concierge medicine. In the ever-evolving healthcare world, let’s not just stick to the status quo; let’s celebrate a Physicians’ leadership abilities, not belittle them for taking a risk, exercising good judgement, seeing a different path forward and sending back road maps and coordinates to follow. Let’s support and uplift each other because, it is no longer about being the best Doctor inthe world anymore, it is about being the best Doctor for the world, for your patient and for your local community.”
Nominators are encouraged to share nominations and perspectives on the initiatives, achievements, and examples of leadership they’ve observed within the past 12-18 months to present a full picture of a candidate and demonstrate what makes them a Top Physician Leader in Concierge Medicine. Final selections will not be announced until mid-2025, at the industry’s trade publication, www.ConciergeMedicineToday.org.
All Top Physician Leaders in Concierge Medicine selections will be prominently recognized in mid-2025 at Concierge Medicine Today online.
“There’s no fee, no payment required, nor an award to purchase. It is recognition only in its purest form,” adds the Editor.
Click to view our online coverage of past recognition by Concierge Medicine Today, supporting the achievements and hard work of Physicians.
ELIGIBILITY RULES
Top Physician Leaders in Concierge Medicine nominees must either work or have worked in or for a concierge medicine practice or served in a leadership capacity for an organization serving the space within the past 12-18 months.
ENTRY DEADLINE
The final deadline for nominations is March 1, 2025. All notifications must be submitted online. Email, social media DMs, and the like will not be accepted.
HOW TO ENTER
If you are NOT a Physician and would like to nominate a Physician to be considered and potentially recognized on the distinguished list of Concierge Medicine Today’s Top Physician Leaders in Concierge Medicine 2025-2026, please complete this online nomination form;
NOTE: Limit one submission per Physician.
If you ARE a Physician and would like to nominate a Physician (or yourself) to be considered and potentially recognized on the distinguished list of Concierge Medicine Today’s Top Physician Leaders in Concierge Medicine 2025-2026, please complete this online nomination form.
NOTE: Limit one submission per Physician.
Disclaimer
Please remember the following information: The content on this website is for informational purposes only and should not be considered a substitute for professional medical advice, diagnosis, or treatment; The website does not endorse or recommend any specific individual, physician, or medical practice; It’s important to always seek the advice of a physician or other qualified healthcare provider with any questions regarding personal health or medical conditions; If you have a medical emergency, please call 911 immediately; The website and its content are provided as-is and the use of any information is at your own risk; The website does not claim that any particular physician, company, medical practice, service, or product is safe, appropriate, or effective for you; Always seek professional medical advice before making any healthcare decisions.
Your last day at work
What happens when a Doctor trades in their old job for a shiny new one, only to discover that the grass isn’t quite as green as they hoped for? Whether you’re contemplating a leap into the world of concierge medicine or just daydreaming about your dream job, there are three simple questions you might want to wrestle with before making any big moves!
Winter 2024
A Sept. 3, 2024, MGMA Stat poll found that 27% of medical groups report having a physician leave or retire early in 2024 due to burnout, compared to 68% that did not and 5% reporting “unsure.” Even more interesting is that a larger percentage of physicians in another survey expressed a likelihood of leaving their current position within the next few years, with some studies showing up to 35% considering a departure.
Whether you’re contemplating a leap into the world of concierge medicine or just daydreaming about your dream job, here are three simple questions you should consider if and when you decide to make a big move in your career!
Who can you turn to for guidance?
We all recognize the value of sound advice intellectually but it's crucial to seek counsel from individuals within your network who won’t simply tell you what you want to hear but rather will support and guide you in making critical decisions and help you identify your blind spots. Think about creating a list of these people and reach out to them. Consider taking them out for lunch and telling them beforehand what you’d like to discuss. This will shorten the pleasantries and help shortcut the discussion around your primary concerns about a job transition.
How much time will it take to heal the emotional and psychological wounds of the past workplace experience?
Emotions often play a pivotal role in our decision-making. However, what will happen in six months when you discover that the new job has its own set of dysfunctional workplace issues? Allow yourself time to heal from the weight of the last workplace experience. There’s nothing worse than finding yourself a decade from now (or perhaps retired) and still traumatized by the same set of emotional wounds you never allowed to properly treat years ago.
Will you take a leap or build a runway?
Financial concerns are not always the primary factor when it comes to changing careers or jobs. Often, it’s about better hours, a supportive boss, or more family time. Many physicians contemplating career transitions tend to overlook the “what if” questions: What if this doesn’t work out? What if I don’t enjoy the area? The list can be endless. When seeking career advice from trusted individuals, be cautious of platitudes. These can create a misleading sense of confidence. For instance, when you share your story, some may advise you to “Just take a leap of faith.” But where is your parachute? What does your financial runway look like if it doesn’t pan out? Others might suggest, “If you build it, they will come.” While these statements may hold some truth, they often lack a foundation in reality. If your next career move doesn’t succeed, what will you stand to lose? What are your exit strategies? How long is the contract? Who will be your actual boss?
Bonus: Here are the five books we encourage any Physician to read if you’re in a season of career transition.
“What To Do Next: Taking Your Best Step When Life Is Uncertain” by Jeff Henderson (Author)
“Necessary Endings” by Henry Cloud
“The Doctor’s Guide to Concierge Medicine” by Concierge Medicine Today (Author)
“Today Matters: 12 Daily Practices to Guarantee Tomorrow’s Success” by John C. Maxwell (Author)
The EntreMD Method: A Proven Roadmap for Doctors Who Want to Live Life and Practice Medicine on Their Terms” by Nneka Unachukwu
Why happy patients tell the best stories.
The new patient referral.
It's elusive. It's mysterious.
You don't always know when they will arrive or even where they come from.
You are glad they are here.
At the end of the visit you still wonder 'why' they chose you?
Name drop from a former patient? OMG! What did they say about me?
Or was a current patient? Google search?
Was it strictly because of location to their home or work that they picked you out of the half-dozen choices around the area?
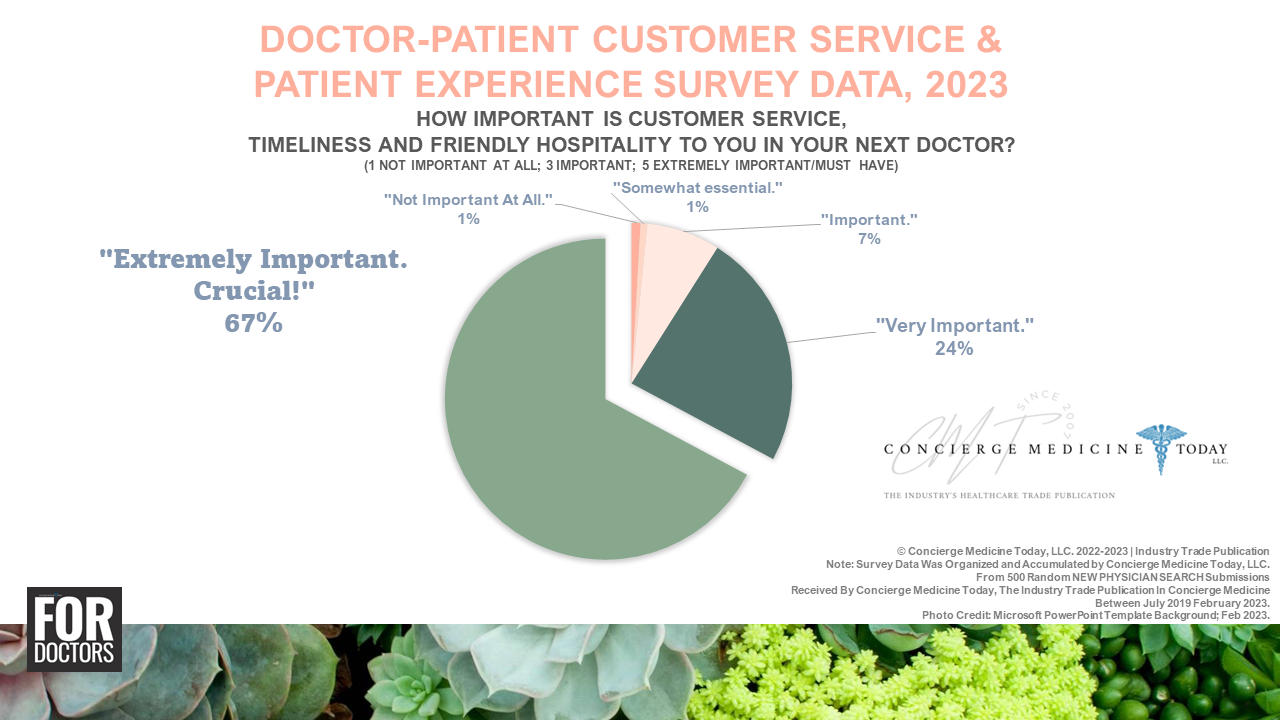
At Concierge Medicine Today over the years, we’ve taken great interest into the how and why of patient decision-making. We took to our online polls and asked our Physician readers and prospective patient readers whom visit our web properties daily and asked them Why Do Patients Love or Leave A Concierge Medicine Physician?
We discovered something interesting.
We learned over the years that it was about the feeling a patient gets when they pick up the phone, make the appointment, talk to the staff, sit down for a conversation, meet with the Doctor and all the follow up afterwards.
It wasn’t just about the Doctor.
It was all the stuff around the Doctor as well.
Rarely was the price tag an issue that prevented the new patient from signing up with a concierge medicine practice.
We dug a little deeper.
When you ask people why they are leaving/have already left their current primary care of family medicine Doctor, for example, they told us three core reasons.
First, 'I felt like a number.'
Second, 'He/she spent less than 15-minutes with me on every visit.'
Third, 'The staff was rude.'
At CMT over the past three years, we asked Physicians, 'How many handwritten notes or handwritten thank you notes do you write to Patients per month?'
32% - "I write between 1-2 per month."
14% - "Between 3-6 per month."
21% - "Between 7-10 per month."
11% - "Between 11-20 per month."
6% - 150+ Thank You Notes/Handwritten Notes Per Month (or 4-5 notes, personally addressed per day).
16% - None. Zero.
One of the most important strategies (and possibly least expensive) that you can and should deploy in your medical practice that literally only costs you a few minutes a day and less than $0.65 to drop in the mail.
As one Physician we interviewed recently on our DocPreneur Leadership Podcast, "It cements the patient-physician relationship and creates positive word of mouth about you for free!"
I love that!
So even if a team member failed to ask the follow up question about how that new walk-in patient found your practice or an inquisitive question about why your current patient told a friend who told you about this place, you can create a positive word of mouth narrative about what's being said about you in your local community.
What Doctor do you know that doesn't want to create a sales force for free?!
If you meet 'em, I'd like to know ‘em. :)
Try writing one handwritten note or thank you note to patient per week. I'll even give you two weeks off for vacation. That means that in one year you will have changed the story or created a story worth people talking about in your local community.
Every team member from this point on should be equipped and at-the-ready when these new patients arrive for the first time. You should then equip your staff to ask 'How did you hear about us?' and then, sit back and listen to the real story about their personal Why behind the actual visit.
I think you'll be surprised at the results, as your peers in Concierge Medicine have been now who have implemented this strategy in their local communities.
A lot of medical administrative staff (and even some Physicians) are afraid to ask patients the awkward 'So how'd you hear about us?' because you don't want to scare them off by seeming too happy that they’re here.
I think we can 'Scale Kindness' in healthcare for the price of a stamp. It starts with you and me!
“My vision is to cultivate a personal Patient - doctor relationship amidst a bustling urban community where impersonal professional relationships are the norm," said Dr. Edward Espinosa of Buckhead Concierge Internal Medicine in Atlanta, GA. "Our practice strives to deliver quality medical care with an emphasis on evidence based medicine, open communication, easy accessibility, and a focus on customer service. These benefits can lead to an overall improvement in how healthcare is delivered and may ultimately improve outcomes.”
It's in these small and memorable moments when they open up a note address to them from their Doctor that you cement your relationship with them. Hopefully for a longtime.
So, one handwritten note per week is the goal.
In the meantime, stop putting so much pressure on yourself. You don't need to visit with every patient for 8-hours or write 50 thank you notes a month. You just need to start with one!
Now, go, get started!
Celebrating patients: 3 missed opportunities Doctors can identify today that will make a dramatic impact on the rhythm of your day.
3 missed opportunities Doctors can identify today that will make a dramatic impact on the rhythm of your day.
By Editor, Concierge Medicine Today
I expect too much of my Physician.
I ask too many questions.
I talk too much, and I consistently get in my head, worry, and overthink things.
Customer service and common-sense hospitality “stuff” really bug me in healthcare.
As a patient, I know how it feels to be passed off to a phone tree, an NP or PA in the practice, or thrown to the [metaphorical] wolves of the billing department.
I know what it feels like as a parent to have my son sit with a Doctor we hoped would be caring, cautious, and updated while you sit on the tip of the chair “concerned,” and in less than five minutes, they drop the standard abbreviations and acronyms and leave without the full story. Then, you find they are now giving more attention to the next chart down the hall, and the patient waiting in the exam room next door gets the laughter, time, and attention you had hoped for.
Patients know what caring, serving, and treating are within seconds. We feel your compassion and understand where this encounter will take us within a minute or two of your entering the exam room or us simply walking into the lobby.
You are known for something in your community.
Yelp! reviews and Google Reviews might tell us exactly "What you are known for ..."
As your practice grows “older” and perhaps your team gets “colder,” we'll pick up on trends in the reviews we read. Some are true. Some are not. We take the good with the bad. Some are informative and constructive and some are just plain rude.
For starters, maybe it's a smile when you walk into the exam room. Perhaps you asked a patient,” How is school going this year?
As we all know from experience in the business of medicine, growth is the bi-product of doing the right things, consistently.
Here are 3 missed opportunities Doctors can identify today that will make a dramatic impact on the rhythm of your day.
1. Be Aware of the climate you bring with you when you walk into the practice.
Author and Speaker Jeff Henderson says, "Every relationship has a climate—sunny, stormy, or even icy. And the current climate dictates the forecast. The problem is that many of us are unaware of the emotional climates we carry around with us. We affect the emotional climate [of the room] when we arrive home or step into a meeting at work. The truth for all of us is that at least one of our relationships could use climate change. And until the climate changes, the forecast will remain the same."
When you walk into an exam room, you bring a climate with you. When you walk in the back door of your practice and greet your staff first thing in the morning, you bring a climate with you.
Pro Tip! Try to start the day with your staff by giving them the courtesy of a meaningful morning greeting!
We all get stuck in our daily routines.
For example, what does your interaction with a staff member sound like if the first thing they do when they see you arrive at the practice is immediately jump into a problem?
These are challenging moments.
What about when you have a disagreement with your spouse in the morning before leaving for the hospital? How do those conversations dictate your mood and “climate” and, potentially, how do you greet the first patient of the day?
How we begin and end our days creates a natural rhythm in our lives.
The goal isn't perfection, it's progress.
If you don’t know how to do this, just start by greeting the first person you see in the practice by their first name, preferably.
Why is the "first name" important you ask?
Well, research says for example … Northwestern University found Doctors do not address patients by name in half of first-time visits, even though nearly all patients want this personal greeting, according to new research from Northwestern University's Feinberg School of Medicine.
“Greetings may seem a rather mundane part of physician-patient communication, but they create a first impression that can affect the chance of developing a therapeutic relationship,” said Gregory Makoul, lead investigator of the study, professor of medicine, and director of the Center for Communication and Medicine at the Feinberg School.
There has been little evidence to guide doctors about how they should greet patients or what patients actually expect. Makoul's study focused on finding out what patients think is an appropriate greeting. He also analyzed a sample of interactions between doctors and patients during first-time visits.
Makoul and his colleagues collected information from 415 phone surveys in which people were asked how they expect to be greeted by a doctor. Researchers also viewed and analyzed more than 120 videos of primary care visits in which the doctor and patient met for the first time.
The study, published June 11 in the Archives of Internal Medicine, reported that 78 percent of survey respondents wanted the physician to shake their hands. Nearly all patients wanted to be greeted by name, including 50 percent by their first name, 17 percent by their last name and 24 percent by both their first and last name. Most patients, about 56 percent, wanted physicians to introduce themselves using first and last names, while 33 percent expected last name and 7 percent expected first name.
Makoul's research team found a striking difference between expectations voiced in the phone surveys and the actual interaction between doctors and patients in the videos. While 83 percent of doctors shook hands in the videos, only half addressed the patient by name.
Source: Many Doctors Don't Use Patients' Names on First Visit; June 26, 2007 | by Marla Paul
To layer more onto the case for support of our topic here on the importance of Doctors greeting Patients, an interview with Ritz-Carlton's former CEO, Horst Schulze in Chief Executive said "We taught our employees no matter what you do, when a guest comes within 10 feet, you look up and greet that guest. If the guest needs help, no matter what you’re doing you help. That’s a culture of ours. That’s what we do. That works in every country. If a guest asks for directions, don’t point. Take them there. That was appreciated ..."
Ricco de Blank, CEO of Sun Hung Kai [Hotel] Properties, which owns Hong Kong’s Four Seasons, Ritz-Carlton, and W hotels, said the following when it comes to customer greetings, first-time interactions, and first-name service.
At Ritz-Carlton, every employee from vice presidents to busboys carried a small folded paper brochure called the “Credo,” a Schulze version of the Ten Commandments, dealing with everything from how to give guests directions to the elevator to treating fellow employees. From the Capella Canon, Number 8 on the expanded 24-point list reads, “Always recognize guests. Interrupt whatever activity you are doing when a guest is within 3 meters (12 feet), greet them with a smile, and offer assistance.”
2. Stay On Time Within 5 minutes and Apologize If You're Late.
"Behind schedule."
These are the two dreaded words of each Physician's day.
It's tough.
You never quite know when the wave will hit you.
It's a complex race to the finish. It's the unnecessary friction you swim against, and it's an annoyance to Patients.
Over time, it widens the gap between you and the Patient.
You're doing your best just to keep up.
Number 18 on the Capella Canon we mentioned above is, “The suggested hours of operation are guidelines, not limitations for satisfying individual guest desires and preference.”
Most medical offices in primary care and family medicine are 9-5 with after-hours and urgent care services built in. Understandable.
Sadly, when you walk into the exam room 45 minutes after you were supposed to, there's not a lot of grace. There's no reason not to address the elephant in the room [eg. you're late]. Most physicians are in such a hurry that they skip over the apology for their lateness and move right into addressing the issue in the room.
The gap widens even further.
Why?
Lack of relationship to be blunt.
Welcoming the Patient by their first name vs. just diving straight into the issue may save time, but it costs you eventually.
Neither side likes this rushed visit.
So how late or how late is too late?
A study done at San Francisco State University found that about 20% of the U.S. population is chronically late–but it’s not because they don’t value others’ time. [But] It’s more complicated than that, says lead researcher Diana DeLonzor.
“Repetitive lateness is more often related to personality characteristics such as anxiety or a penchant for thrill-seeking,” she says. “Some people are drawn to the adrenaline rush of that last-minute sprint to the finish line, while others receive an ego boost from over-scheduling and filling each moment with activity.”
Author Charles Dickens once said, "I never could have done what I have done without the habits of punctuality, order, and diligence, without the determination to concentrate myself on one subject at a time."
DeLonzor says that 45% of everything we do on a daily basis is automatic: “Our lives are filled with habits–from the way you brush teeth to how you get dressed and leave for work,” she says, adding that they’re necessary. “If we didn’t do things automatically, it would take us forever to get through our day.”
The habits of people who are always on time are highly structured. They analyze their daily activities, set routines, and stick to them on a regular basis. Chronically, late people, however, don’t have structure and often fall on the attention deficit disorder spectrum, says DeLonzor.
“Instead of thinking about why their routines don’t work and trying something different next time, chronically late people simply hope that tomorrow will be better,” DeLonzor adds.
To become punctual, DeLonzor suggests putting more routines and structure into your life. For example, do everything you can to prepare for the morning the night before.
FOR PATIENTS, according to Esquire Magazine,
DOCTOR’S APPOINTMENTS
You are always encouraged to show up fifteen minutes before your appointment time, so that you can take that filthy clipboard with the Lyrica-logo pen attached and fill out a million forms. But, especially while you’re young and your medical issues are relatively few, it turns out you can do that pretty quickly. Then you’re stuck on a leather couch watching House Hunters International until fifteen minutes after your appointment time. Nuts to that. You can push it a little bit here. Time spent in a doctor’s office is time spent contemplating your mortality, and it behooves you to minimize it.
THE RIGHT TIME IS FIVE MINUTES BEFORE THE SCHEDULED TIME, JUST IN CASE THERE’S SOME WEIRD ISSUE WITH YOUR INSURANCE.
“We must not be distracted from the four supreme objectives of any organization that wants to succeed: 1. Keep the customer. 2. Get new customers. 3. Encourage the customers to spend as much as possible!—but without sabotaging Objective Number One. 4. In all of the above, keep working toward more and more efficiency.”― Horst Schulze, Excellence Wins: A No-Nonsense Guide to Becoming the Best in a World of Compromise
One final thought from a Physician on this topic when she told me … "Years ago, I once had a patient send me a bill for her time as I was running 90 minutes late. That's the day I thought long and hard about my schedule made some leadership changes and shifts in my practice, and told myself, 'Never again.' Honestly, I was more ashamed than angry. She was right. I had disrespected her time. I valued my time as more important than hers and it was a chronic condition. As I said earlier, I’m occasionally late when I walk into the exam room. Sometimes, a true emergency happens, or an outlier event transpires. When it does happen, I try to give a very detailed account of why I was late to every Patient for the rest of the day, apologize profusely, asking forgiveness ... which, by the way, not many Doctors do, and that's the key ingredient to the process. Without it, you just piss people off. I then make sure the other person knows I'm sorry and that I take their time very seriously, and assure them it won’t happen again."
Timeliness is hard. Timeliness is good and the good stuff is always hard.
The goal isn't perfection. The goal is progress.
RELATED STORY
The Etiquette Rules of Being on Time
3. Look For Everyday Moment to Express Your Gratitude To Your Staff and Patients.
If you see your staff do something out of the ordinary and kind to a patient or coworker, acknowledge it.
Handwritten notes haven't gone out of style.
Saying something right then is also good. Don’t stop there.
People need to know their Physician is paying attention. Whether it’s a colleague or a patient, we want to know you care.
We need to know you’re watching.
It doesn’t have to be some grand gesture, just something unexpected.
If you really want to surprise a coworker, for example, write them a note at the end of the day. Handwrite the envelope and address it to their home.
Sure, you could leave it on their keyboard or their chair for them to find the next morning. That’s nice but mailing it to them directly to find a few days later is even better. It informs the receiver that you thought about them and cared enough to take 90 seconds out of your busy day to acknowledge only their actions.
This can apply to your spouse. He/she is your cheerleader. In some ways, they are a vital component of a Doctor's office. They’ve helped you with your career choices, and whether they work in the practice or not, they deserve some recognition, too!
Often, we hear from Physicians about how their spouses sacrificed to help them become who they are today. Finding a quiet moment to write them a note that rewards them with a gift of gratitude is priceless.
“Notice what your wife does regularly for you and take a moment to say thank you for it,” said one psychologist we spoke to recently about implementing a gratitude system in a medical practice. I noticed something the other day. I made dinner (which I probably do about once a week) and when we sat down to eat, my kids said, ‘Thanks, Mom; this was great.' It made me feel good. But you know what? I make dinner the other six nights a week and no one ever says 'thank you' or even acknowledges it."
Your spouse, your coworkers, and your patients may get the best part of you eight to twelve hours of every day. It's important to recognize what others do regularly for you and thank them for it the other 12 hours, too!
Just a thought.
“If a person is breathing, they need encouragement.” ~T.C.
Over the next few months my hope is that as Physicians reading this book, regardless of specialty and busy schedules will take a moment each week and handwrite a personal note to a colleague, coworker or a Patient.
This small, random act of kindness may take the form of a blank card, a piece of stationary, a thank you card or a greeting card.
It can be something simple. There's not a template here. As long as what you write uplifts and encourages someone.
Every hardworking healthcare worker could use a little encouragement or a note from an old friend or a fellow colleague.
Truett Cathy, the founder of Chick-fil-a once said “If a person is breathing, they need encouragement.”
Chances are pretty good that if you’re reading this, you’ve not written a handwritten note to a friend, your spouse, a patient or a coworker in quite a while, if ever.
I'm here to tell you that the evidence is in your favor here.
According to the New York Times, June 2023 in an article entitled Gratitude Really Is Good for You. Here’s What the Science Shows by Christina Caron. In the article she writes “Two decades ago, a landmark study led by the psychologist Robert A. Emmons sought to understand how people benefit from gratitude, a question that scientists had rarely explored until then.”
Meaning, 'gratitude is good for the giver.'
Author and communicator, Jeff Henderson in his book What To Do Next: Taking Your Best Step When Life Is Uncertain, said it best when he writes “The best form of momentum is a more emotionally healthy you. In fact, the more emotionally healthy you are, the better investigator you will become because you can spot the momentum in your life easier.”
I know this idea may appear soft and vulnerable to some of you. I know most of people working in healthcare will dismiss this as a good idea but you just don’t have time to for it.
As Henderson writes “The scariest place to be is the same place as last year. No growth, no challenges. Just the same.”
Don't Do Nothing.
Every day we get private messages, texts and phone calls from Doctors all over the country (e.g. United States mainly, but on occasion, a few other countries too!) telling us that they are just plain burnt.
“If a person is breathing, they need encouragement.”
~Truett Cathy, Founder, Chick-fil-a
That's a terrible place to be. They've often lit the candle at both ends and not only are they frustrated but they're relieved that maybe, just maybe, they've found a potential business model or a lifeline [in Concierge Medicine; VPN; DPC; etc.] that could have a significant impact on the rest of their career and future in medicine.
In a profession that’s tough, albeit impossible, let’s provide a little encouragement to those around us. Let’s not let another day pass without dropping a note in the mail to a colleague [or Patient].
Steve Green in 2014 said something really great. He said ... “Encouragement is never small when you’re on the receiving end.”
What are you waiting for? Grab an envelope, a card or a piece of stationary and a pen and get started.
$21 bill sent to collections sends the wrong message [to patients]
“We attempted to contact you three times,” is what the Office Manager at the clinic said to the mother of two when she called because of the threat of being sent to a collections agency.
Every one of your Patients needs a small deposit of your time, over time, not a collection notice.
It’s not amount that bothers me. Medical offices need to get paid. They serve an important function in our communities.
My problem isn’t with the patient, nor the office manager.
My problem is with the lack of relationship between the medical office and the patient that could have prevented this story from ever being told, nor written about.
This kind of action is taken every day. Probably hundreds of times per day across our country.
You and I both know there is no 'thank you' from the medical practice down the street when you pay the bill before the deadline.
And, we've probably never received a 'thank you' for paying that car payment on-time for the past several months. Nor is there a parade or a bass drum fan-fare from the mortgage company or hospital for paying the bill, on-time, again.
Instead, patients are greeted with silence.
Nothing,
Until, you're a few weeks later when the insurance EOB hasn’t been updated online and the Doctor’s accounting office sends out its routine monthly statements to patients.
The the #$@&! hits the fan, right?
We have all received PAST DUE notices, even from our own Doctor.
They provided a service. It worked and you owe the money.
In today’s impersonal healthcare culture riddled with insurance, bureaucracy, late notices, customer no service hotlines and unhelpful, impractical phone trees the medical office willing to be different is the one that is going to last the longest in our communities.
Why?
Because people know them, like them and trust them.
And isn’t it true that if we know you, like you and trust you, patients respect you enough to pay their bill.
Now, there’s always those and a percentage who will take advantage and that’s to be expected and anticipated. You need to have a process for that.
But if you have to look at a medical chart every time I come to your practice and you’ve been my Physician for the past 15-years and you send a mother a threatening collections letter for $21 there is a relational problem, not necessarily an accounting problem.
When a medical office sends one of these dreadful notices that says something like 'Your urgent attention is required. To prevent collection efforts and additional costs such as attorney fees, please remit payment in full...' where is the relationship between the Patient and the Practice heading?
What is even crazier is to think we all sign-up for the next appointment before we leave so we can start this [frustrating] process all over again?
Her'e’s one true story from a concierge medical practice in Ohio.
"Before I opened my [Concierge Medicine] practice I used to dread the calls to collect the unpaid payments in my practice. My staff hated those calls and even worse, knew that by sending out those letters, arguments would ensue. It was always a struggle. It created tension between my staff and my Patients. But today, it is much easier. The secret I discovered was I starting using 'thank you' notes. I know, it sounds silly. I wrote thank you notes to my patients. They were short and sweet and in some cases for the most random things."
I will conclude today with this final thought.
Every one of your Patients needs a small deposit of your time, over time.
Take the time to care about what’s going on in their personal lives. By caring you are serving your community of patients to! A random act of kindness in a handwritten, short note that’s then sent via USPS mail to them with you writing their name on the envelope will surprise them and you’ll be a [metaphorical] rock star!
This is important, not only because it creates a closer bond with your existing Patients, but it helps them help you. They will soon be telling their friends and family about how special their Doctor is.
Patients are going to tell a story about you when they leave your office.
What story do you want them to tell?
I hope it’s not about a $21 letter that’s soon going to be sent to collections when the patient is simply waiting for the insurance EOB.
I think healthcare offices can do better.
Oh, and PRO TIP! This can work with your staff too!
PS - Food for thought ... If you have a TV in your medical office, please be sure you are using it. At the very least, run some educational slides about your practice or have age appropriate content on. Be mindful, little eyes may be watching too! For example, we visited an UCC in Atlanta recently and noticed the lobby had inappropriate content on for children and yet, dead silent tvs in the exam room. The DMV however, had educational slides about how to make their process easier. So, DMV = 1; Doctor's Office = zero.
Leaving your job [in healthcare] on a high-note.
A lot of Doctor’s have quite the colorful tale of woe when it comes to their previous jobs.
Some really good people worked with you despite the atmosphere or toxic work environment. They are the ones you will hopefully remember one day when all of what you've accomplished in healthcare becomes just another story you tell your friends and family. Or will they?
From stressed out to burnt out, it’s rare you meet a Physician without a adventure-filled story about their past, right?
My question for you today is simply this … What version of the story will you tell your family and friends one day about this moment in your career, right now?
Will you be the hero that slayed all the dragon and showed that insurance company or gave that hospital administrator or board a mouthful or will you look back with fond recollection of the people you worked next to under stressful conditions? Or, will it be just the patients you cared for and served that come to mind? Or for some, dare we say many, will you roll out the wheelbarrow of stones, throw a few around and carry that mental and emotional baggage around like it’s your pet?
The latter is where a lot Physician’s we run into at medical conferences and group settings. Whether they worked at the hospital, some clinic, an urgent care, or “that practice” usually the story they tell is filled with ups, downs, twists and turns and ultimately ended with years of anger, bitterness, resentment and regret.
What’s worse is, they carry this mental and emotional anger and bitterness for years, if not decade. It impacts their decisions until this very day. And, if you were to ask them if they’d want their kids to follow in their footsteps, they’d usually say “I sure hope not. Please, don’t be a Doctor.”
That makes me sad.
What’s sadder than all of that is that some of the Physician’s you and I have encountered in those dark and quiet hallways of the hospital or sometimes closest to the open bar at CME events, will paint a colorful adventure and spin quite the yarn where they were the hero against the insurance company, gave the administrators a earful and showed those bureaucrats who you really were.
That’s all well and good. Honorable perhaps. But not the point I’m trying to make.
The point is that ultimately all of these stories end up as a story one day. The real question they should be asking themselves is, what story do that want to tell? Or, do they prefer to carry these chapters around as baggage and enjoy rolling out the wheelbarrow full of pain and anger, bitterness and resentment.
We know these people. Perhaps they are our friends. Maybe part of our family.
The story was tragic. They were done wrong. And yes, it wasn’t fair what happened.
Even if they “let you go” or “you had to leave” … is that the weight you really want to carry around for the next couple of decades?
I’m sure for most of you, it’s not.
To finish well, don’t burn bridges.
Easier said than done, right?
We’ve all been taught this adage from an early age. We might even agree with it. We’ve all probably informed our kids about it and hope they’ll do the same.
On the other side of that sentiment however is you and I wrestling with a lot of hurt feelings, betrayal, not enough compensation, long-hours, mistakes, should haves, wish I could haves, bitterness and a lot of resentment that took years from you.
It’s easy to think, “I’ll never work with these people ever again.” And, depending on the situation, it may even feel good to burn a bridge or two on your way out. After all, they burned you first, right?!
A recent article published by the Global Leadership Summit written by Jeff Henderson, Author, Coach & Consultant and Founder of The For Company says “But don’t forget, when you burn a bridge the person who is most often burned is you. Take the high road even when others don’t take it with you.
Here’s another great question to consider by Your Move where the speaker said “Along the road of life, we all pick up some baggage. But how do you keep the ghosts of your past from showing up in your future?”
“The truth is leaving well is something that takes time. It doesn’t start when you put in your two-week notice. It’s far deeper and more challenging than that. Finishing well requires planning. Finishing well requires vision. Finishing well requires humility. Finishing well requires character. We honor the organization and the people we’ve served by finishing strong.”
~Global Leadership Summit, Jeff Henderson, Author, Coach & Consultant and Founder of The For Company
The point I’m trying to make here FOR Doctors who don’t want to spend years or decades of their life telling stories where they’re the hero and everyone else is the villain is you and I can avoid that mental and emotional fatigue by finishing our current season well.
How do you finish this job or this chapter or season of your career on a high-note?
Simple, finishing well requires expressing gratitude.
As Henderson put it (above), “Finishing well requires planning. Finishing well requires humility … and character.”
For some Physician out there right now wrestling with indecision about whether he/she should stay or go, finishing well may just be the most important test they face. Do you leave your co-workers with a “thank you” note or the middle finger?
One last story to help wrap it all up.
Henderson provides us with one last practical real-life example that we hope may inform your next step if you’re a Physician in career transition. He said “Over the course of my last six weeks at Gwinnett Church, I wrote over 120 thank you notes to staff members there, and at North Point Ministries. I mailed them my last day. It was just a small way of saying thank you one final time, and one additional way to honor them individually.”
And finally, if all this just sounds a little too squishy for you … consider this:
Science confirms it mattered. Studies show that employees who feel appreciated are happier, more engaged, more productive, and more likely to contribute in positive ways. And it's not just the recipient who benefits. Studies show that people who express appreciation are more optimistic, as well as physically and emotionally healthier. In other words, gratitude stays with those who give it.[1]
[1] (Source/Credit/Author: INC. LIFE Home Depot's CEO Did This 25,000 Times. Science Says You Should Do It TooHere's a simple and effective leadership tool that is quickly becoming a lost art. EXPERT OPINION BY ELISA BOXER, JOURNALIST AND MINDFULNESS COACH @EBOXER; NOV 10, 2017; https://www.inc.com/elisa-boxer/home-depots-ceo-did-this-25000-times-science-says-you-should-do-it-too.html)
Shaming and degrading peers: There’s no more room [in healthare] for mean tweets and echo chambers.
Wikipedia defines the echo chamber effect as 'The echo chamber effect occurs online when a harmonious group of people amalgamate and develop tunnel vision. Participants in online discussions may find their opinions constantly echoed back to them, which reinforces their individual belief systems due to the declining exposure to other's opinions.'[2]
You know you've entered (or exited) an echo chamber in healthcare if you slink back in your chair after thoughtfully and quietly listening to several audience members (or speakers) all day and you’ve heard the cheers from the audience and listened to the types of comments they’ve made during the break. You think to yourself, 'If they only knew what I do or who I work for ... I would be run out of this place.'
Evangelism, not the religious kind, but the “rah-rah” kind isn’t new in healthcare. It's interesting to me as a writer, an advocate FOR Doctors and an observer or student of healthcare musings out there that the amount of rants by Physicians, grumpy editorials by some healthcare journalists and even former Physicians are pushing their opinions like sales pitches on LinkedIn comment threads or “X” (formerly Twitter) and repeating the same tired points about how broken healthcare is and how they have all the answers.
Years ago in college one of my communication courses discussed platitudes and echo chambers. I think this conversation is helpful and relevant for healthcare, even today.
Oxford Learner's Dictionary defines platitude as 'a comment or statement that has been made very often before and is therefore not interesting'.[1]
Wikipedia defines the echo chamber effect as 'The echo chamber effect occurs online when a harmonious group of people amalgamate and develop tunnel vision. Participants in online discussions may find their opinions constantly echoed back to them, which reinforces their individual belief systems due to the declining exposure to other's opinions.'[2]
Platitudes in healthcare are like the hair on our head. They’re everywhere, or maybe for some of you, they used to be.
For example, one popular medical publication writer wrote ... They should create more access points and include opportunities to address the drivers of health.
If we dive deeper into some echo chambers in healthcare we've probably attended without knowing it was one … a few medical conferences over the years and you thought to yourself on the plane ride home, 'Wow. I can’t believe they said that.'
ECG's principal Dr. Nick van Terheyden writes Changing healthcare in the US will require different thinking and ideas. But many of us are guilty of being stuck in our own echo chambers—interacting every day with the same people at work, in social settings, and at conferences.
The Editor of the American Association of Neuroscience Nurses, DaiWai M. Wilson wrote an editorial in April of 2020, Vol. 52, Number 2 entitled "The Dangers of Echo Chambers in Healthcare."[3] In the editorial he writes, Echo chambers likely exist [in healthcare] because they boost self-confidence. Talking to people who think like I think is very comforting. Being reassured that I have been right all along makes me feel good. Echo chambers bring a sense of fellowship and belonging. He concludes his editorial with these thoughts, ... whatever you write must be clearly written and supported by peer-reviewed evidence.
Where your perspective and mine about a few things in healthcare may divert from these places and faces in healthcare may quite possible sound like this … ‘I shouldn't have to agree with you to work alongside you in healthcare and be effective, yet right now, you're wanting me to pick a side or agree that you're right when I'm just not there yet.’ Personally, I am of the persuasion that how you and I treat people, talk about a patient, a payor, a nurse, a hospital, a system, talk to or respond to opinions that differ from our own and care for one another is our true identifying mark, not be ostracized or fear ridicule because I simply don't agree with you.
Triumph Kerins and Sekoul Krastev in September of 2022 wrote a really insightful and interesting article to peers entitled Escaping the Echo Chamber: How to Build Safe Peer-to-Peer Mental Health Platforms.[4] In the article, they write The main issue with peer-to-peer mental health communities is that they can turn into echo chambers – environments where beliefs exist unchallenged and are reinforced by the group, regardless of validity or accuracy ... Paradoxically, it is the same factors that make peer-to-peer online communities such an effective mental health tool –ease of access, normalization, and trusted peers– that occasionally make way for destructive behavior patterns.
I highly recommend you check the article referenced out. It was an insightful read on mental health and the effects of echo chambers.
I say all of this to say just one thing, be kind and open-minded to one another.
Particularly if you’re the one who finally recognizes you were one of the ones in the audience “rah-rahing”.
Working in and trying to change the world of healthcare today is extraordinarily challenging enough without mean tweets, derogatory blogs and putting a colleague down just because they deliver healthcare a bit differently from you. We don’t need more of people, your colleagues, a few of your peers or even speakers selected for certain medical conferences stating that their way is the best way to follow. Be open-minded for goodness sakes. Recognize that we all have a boulder we’re trying to push up the metaphorical mountain in healthcare and in our local community. For me, try waking up everyday and going to work and talking about the importance of customer service in healthcare and trying to find exemplary examples of that … and then sharing and telling those stories. Each day I envision pushing my burden/boulder in healthcare up the Wasatch Bench just outside Salt Lake City, Utah where I spent most of my elementary and junior high years starting at these mountains. Sometimes we’ll have people like you who is reading this come alongside and lend a hand. Other days, it feels like we’re all alone on the mountain. Isolated. Abandoned. Doing it for no reason.
If you've ever been there you know the steep slopes, the white caps up at the highest parts and how even in the summer there is still snow up there on that mountain. There will be days we’ve reached a sunny valley and other days we encounter storm clouds that seemingly came out of nowhere. We all have a goal, a mission we’re trying to achieve in healthcare by the end of our career.
As a kid, I grew up spending a lot of time wondering what it'd be like to be on that mountain.
In closing, don’t be the guy or gal who thinks he/she has all the answers and puts others down. We all blaze our own trail on the mountain. We all push our own boulder up the mountain here in healthcare. Believe it or not, we all feel alone a lot of the time, even Doctors. And yes, even when we’re surrounded by our colleagues or Patients we can feel all alone.
If a Patient was to read your comments, your posts [and that day is coming], would it change their opinion of you as their Doctor?
I get it, it’s tempting and easier to be a participant in the echo chamber. You may feel overwhelmed by emotion, comment on that thread or even affirm a colleagues rant and then share it. But please, consider what boulder they’re trying to move. Maybe it’s personal. Maybe it’s professional. The world of healthcare, especially those in primary care and family medicine needs more helping hands. So please, be kind and be considerate to those whom share your degree.
I'll leave us today with two wise statements. One from Gandalf the Gray in Lord of the Rings to his good friend and travel companion Frodo where he says ... "It's a dangerous business, Frodo, going out your door. You step onto the road, and if you don't keep your feet, there's no knowing where you might be swept off to."
The other from my pastor … “We didn’t sign up for easy. We signed up for worthwhile.”
Citations
https://www.oxfordlearnersdictionaries.com/definition/american_english/platitude
https://en.wikipedia.org/wiki/Echo_chamber_(media)
https://journals.lww.com/jnnonline/Citation/2020/04000/The_Dangers_of_Echo_Chambers_in_Healthcare.1.aspx
© 2024 Concierge Medicine Today, LLC. ("CMT") All rights reserved.
Disclaimers: All content presented here is for general information purposes only. It is NOT intended to provide medical, legal, professional, accounting or financial advice. No warranties or guarantees are assumed and user(s) release Concierge Medicine Today, LLC and its agents, representatives and guests from all damages, liability and/or claims. While some of our speakers may be licensed Physicians, they are not your Physician. Please consult your Physician related to anything you may have read or heard or have questions about or call 911. The views, thoughts, and opinions expressed are the speaker’s own and do not necessarily represent the views, thoughts, and/or opinions of Concierge Medicine Today, LLC. The "Concierge Medicine Today, LLC" name and all forms and abbreviations are the property of its owner and its use does not imply endorsement of or opposition to any specific organization, product, or service. Additional disclaimers, releases terms and conditions apply to this content, https://conciergemedicinetoday.org/tcpp/.
History of Concierge Medicine in America (1996-Present Day)
It all begins with an idea.
A History of Concierge Medicine (1996-Present)
Last Updated: January 2024
We love that quote around here. It crystalizes how we feel about you and those who have worked so hard in healthcare to improve it over the past 20-years. To that end, history is important to all of us. We learn from it and we many of our futures are shaped by it. And, a lot has happened in the past 20+ years in healthcare. Author and pastor, Andy Stanley in his book Deep and Wide wrote "We don't drift in good directions. We discipline and prioritize ourselves there. ...often, stepping outside your comfort zone is not careless irresponsibility, but a necessary act of obedience."
What stands out in that quote is that in all of our careers in healthcare it is that our place in healthcare today is the accumulation [or drift] of a lot of little decisions that added up overtime. It is virtually impossible to capture every moment of history into one document or on one page. Concierge Medicine is so wonderfully colored by so many people and looking back [and forward] it has undoubtedly left an impression [for better or worse -- depending on your viewpoint] on our healthcare marketplace.
We felt it was important this year to summarize again some of the noteworthy moments from the past 20-years or so from this industry in two educational and helpful ways. First, by memorializing some of the most educational insights and quotations that have come from Physicians, consultants, on-lookers and others working in healthcare. Second, to have an abridged historical timeline of events and voices that have helped cement the private-pay and membership medicine models into our vocabulary and our culture.
Editor's Note: This is by no means an all-inclusive, every single detail about all of the things that have occurred in this unique healthcare delivery space. It is a summary of many of the highlights however. When possible, we've tried to provide links to the stories, web sites, press releases, research, studies and organizations for you to learn more. We recognize a lot has happened in the past 20+ years. And, it’s virtually impossible to capture every moment in one document or on one page. It's also important to note that within the past 5 to 10 years here in Concierge Medicine and Subscription-based healthcare delivery have been some the most eventful years in the space of Concierge Medicine which have helped cement the private-pay membership medicine model into our vocabulary. More news of Physician's entering this space and educational headlines continue to circulate across the news wire. From The New York Times to The Wall Street Journal and everywhere in between, Concierge Medicine is now a a familiar term that Patients and Physicians alike are learning to understand why this is an important part of our healthcare ecosystem. Finally, as you may be aware, this document is routinely updated, may have imperfections, but we at Concierge Medicine Today, LLC., do our best to routinely edited, correct and keep this 'Abridged History of Concierge Medicine' updated each year as accurately as possible with links to the original sources if we can find them. Therefore, if we missed something or you think we should add something, please, let us know by emailing us directly at editor@ConciergeMedicineToday.com. Thank you!
Abridged History Of Concierge Medicine And The DPC Healthcare Marketplace.
1996: Dr. Howard Maron and Scott Hall, FACP established MD2 (pronounced MD squared) located in Seattle, Bellevue, WA and Oregon. They charged an annual retainer fee of $13,200 and $20,000 per family.
1999: Medical Professionalism Project-consisting of members of the internal medicine community, including representatives of ACP and the American Board of Internal Medicine, set out to draft a charter that could serve as a framework for understanding professionalism.
1999: Institute of Medicine releases the now famous report of medical errors, Patient safety, and professional integrity that caused further probing in physician exam rooms.
2000: Virginia Mason Medical Center in Seattle, WA began operating concierge medical services within its facilities and used some of the profits from the 5 physician practice to subsidize other programs and indigent care services.
2000: MDVIP, founded by Dr. Robert Colton and Bernard Kaminetsky, in Boca Raton, FL. A brand of Concierge Medicine practice and management firm which has set-up more than 700 concierge medical practices with offices in almost every State across the U.S. Update: In April 2014, Procter & Gamble announced the sale of MDVIP to a private equity firm, Summit Partners.
2001: American Medical Association writes concierge physician guidelines: PRINCIPLES OF MEDICAL ETHICS.
2001: July 04, 2001 · Seattle Post Intelligencer Seattle Post Intelligencer In Retainer Medicine, the Doctor is Always In; The idea started five years ago when Dr. Howard Maron, former team doctor for the Seattle SuperSonics, started MD2 (pronounced "MD squared") with his partner, Dr. Scott Hall ...
2002: ACB Foundation , ABIM Foundation and the European Federation of Internal Medicine defines ethical principles and responsibilities contracts between Patient and physician, which is in a language that suggests both parties have equality, mutual interest and autonomy.
2002: Medicare addresses Concierge Medicine and retainer fees.
2002: Centers for Medicare and Medicaid, CMS, outlined its position on concierge care in a March 2002 memorandum. The memorandum states that physicians may enter into retainer agreements with their Patients as long as these agreements do not violate any Medicare requirements.
2002: Pinnacle Care establishes Patient care with a one-time membership fee for access to VIP service.
2002: The AMA counsel on medical services issued a report in June 2002 on Special Physician-Patient contracts. It concluded that retainer medicine was a very small phenomenon.
“When you think of Andy Griffith-style medicine, the doctor had a clinic in the local town. It’d be strange for him to say, ‘What kind of insurance does Opie have?’” ~Editor in Chief, Concierge Medicine Today
2003: American Society of Concierge Physicians was founded by Dr. John Blanchard. The association later changed its name to SIMPD, Society for Innovative Practice Design.
2003: AMA issued guidelines for boutique practices in June 2003.
2003: Department of Health and Human Services rules the concierge medical practices are not illegal and the federal government the OIG, Office of the Inspector General, takes a decidedly hands off approach.
2003: American College of Physicians writes doctors struggle to balance professionalism with the pressures of everyday practice.
2003: June 2003 the AMA Council on Ethical and Judicial Affairs outlines guidelines for “contracted medical services”. The AMA House of Delegates approves these guidelines.
2004: GAO, General Accountability Office writes 146 concierge physicians in the U.S.
2004: Harvard University study finds that 55% of the respondents are dissatisfied with their health care, and 40% of that 55% agreed that the quality of care had worsened in the previous five years.
2005: The AOA, American Osteopathic Association adopts not to recommend and an official policy on concierge care.
2006: MDVIP, a concierge physician practice management firm, reports that 130 physicians within their network treat up to 40,000 Patients worldwide.
2007: Concierge Medicine Today, a concierge medical news agency opens its doors to be an advocate for news pertaining to the Concierge Medicine, retainer-based, boutique, private medicine and direct care industry.
2007: The term "direct practice" was first used in legislation in Washington in 2007 that clarified these practices were not insurance companies under state law-but they do provide basic, preventive medical care.
2008: Boasting an estimated 35 concierge physician practices, Orange County, CA appeared to be a leading hub of Concierge Medicine.
2008: Concierge Physician of Orange County (CPOC) – a non-profit group of existing concierge physicians was founded.
2009: Concierge Medicine Today (CMT) announces the formation of The Concierge Medicine Research Collective, a analytics and advisory arm of CMT based in Atlanta, GA USA.
2009: Concierge Medicine Today reveals that concierge medical practices across the U.S. are thriving in a recession.
2009: Procter & Gamble Acquired MDVIP in 2009 - No less a respected corporation than Procter & Gamble (NYSE: PG) has staked out a major presence in Concierge Medicine. In 2007, P&G acquired a 48% stake in MDVIP, a Concierge Medicine company that was formed in 2000. Then, in December 2009, Procter & Gamble acquired 100% ownership in MDVIP for an undisclosed sum. This acquisition was reported by Dark Daily. (See “Boutique Medicine Venture Generates Marketing Intelligence for Procter & Gamble,” April 5, 2010.)
2010: SIMPD reorganizes, expands its vision, and rebrands itself the American Academy of Private Physicians (AAPP).
2010: Concierge Medicine Today reveals the affordability of concierge medical and private medicine practices across the U.S. stating that over 62% of the programs offered to Patients cost less than $135/mo.
2010: American Academy of Private Physicians (AAPP) forms first local chapter in Orange County, California called AAPP,OC (formerly CPOC)
2010: According to a 2010 American Academy of Family Physicians survey, three percent of respondents practice in a cash-only, direct care, concierge, boutique, or retainer medical practice.
2012: December 2012 - Study Proves Dramatic Reduction in Hospitalizations & $300 Million Savings for MDVIP’s Personalized Healthcare Model
2013: Three Year Analysis of Concierge and Direct Care Medicine Shows Encouraging Signs For Boosting Primary Care In U.S. Economy. Data collected from Concierge Medicine and DPC doctors show encouraging signs across the U.S. from December of 2009 to December of 2012.
2013: New Data on Concierge Medicine Physician and DPC (DPC) Clinician Salaries and Released by Concierge Medicine Today. Data also looks at career satisfaction among Concierge/DPC physicians.
2013: On August 2, 2013, the Dare Center, Seattle, WA, invited concierge physicians, hospital administrators and medical center executives from across the country to participate in a roundtable discussion. This inaugural event took place at the Washington Athletic Club in Seattle.
2013: Family Physicians, Patients Embrace DPC ... AAFP Recognizes Benefits, Creates DPC Policy
Is it worth it?
Since concierge medicine is not insurance (it wouldn’t cover a trip to the hospital) many patients combine it with a high-deductible plan. Concierge Medicine Today, the industry trade publication suggests that consumers think of health insurance more like auto insurance or fire insurance; it should be used for emergencies, not the day-to-day. You wouldn’t use car insurance to change your oil, rotate the tires or buy wiper blades. In the best-case scenario, the sum of the concierge fee ($150/month, for example) plus the bare-bones premiums for a high-deductible plan ($110-ish, theoretically) would pencil out to less than $328 per month, or what the Department of Health and Human Services cites as the “average” cost of health care. ~Comstock’s Magazine, April 1, 2014
2013: The DPC Trade Journal Launched by Concierge Medicine Today. The sister publication, The DPC Journal works directly and indirectly with physicians, businesses and leaders, journalists and the media in the healthcare marketplace to help promote the distribution of news and information, policy initiatives and to reach out to physicians throughout the United States. DirectPrimaryCare.com.
2013: First National Gathering Focused On DPC (DPC) Held In St. Louis: October 11-12, 2013.
“This is the first national gathering of businesses and individuals interested in DPC,” says Dr. Erika Bliss, a Family Physician at Qliance Medical Group of WA and President/CEO of Qliance Medical Management Inc. “DPC is quickly becoming an important contributor to the transformation of our nation’s healthcare system. This conference will bring together key stakeholders to learn more about DPC and discuss its place in the future of medical care delivery.”
“The DPC National Summit will bring together physicians, business leaders, policymakers and others from across the country,” added Bliss. “DPC providers and supporters share the common goal of contributing meaningfully to the improvement of healthcare for all, and by building connections among like-minded people; we hope to accelerate progress toward that goal.”
Overall, Concierge Medicine and DPC are thriving in major metropolitan markets. Four states that have a huge lead in the amount of active concierge or private-pay physician’s in practice as well as consumers seeking their care are: Florida, California, Pennsylvania and Virginia. Each of these States have a significant number of people, most are over the age of 50, seeking out Concierge Doctors and cash-only options. Fortunately, a sizeable number of Concierge Doctors are available to serve them, which is not the case in the more rural parts of the country.
Of great benefit to consumers, prices are dropping significantly due to increasing competition among physicians entering the marketplace, retail medicine pricing, price transparency demand from Patients and uncertainty about the implications of the Affordable Care Act. The Affordable Care Act has also created quite a bit of uncertainty among both Patients and doctors. The shoe has most certainly dropped and now more doctors than ever are considering a career in Concierge Medicine, DPC and retail healthcare.
2014: New Association Formed, American College of Private Physicians (ACPP): Group to Focus on Credentialing Doctors, Advocacy to Employers, Unions, Government and the like to benefit industry nationwide.
2014: P&G sells concierge medicine unit: P&G CEO — ‘Since returning as CEO last year, A.G. Lafley has said P&G will exit ventures that won’t help it grow.’
2014: MD² commemorates 18 years of practicing highly personalized care; March 7, 2014
2014: MDVIP to be Acquired by Summit Partners — ‘MDVIP will continue to be run as a stand-alone company …’ [May 2, 2014]
2014: IRS asked to clarify HSA rules in letter: On June 17, 2014, Members of Congress wrote Commissioner of Internal Revenue John Koskinen asking for clarification on how the Internal Revenue Service (IRS) treats DPC Medical Homes with regard to Health Savings Accounts (HSAs). Senator Maria Cantwell (D-WA), who authored ACA Sec. 1301 (a) (3), allowing DPC practices to participate in health exchanges with Qualified Health Plans, took the lead on the letter and was joined by Senate Budget Committee Chairman Patty Murray (D-WA) and Rep. Jim McDermott, MD (D-WA), ranking member of the Ways and Means Subcommittee on Health. The three WA state lawmakers point out that The ACA rules on the Establishment of Exchanges and Qualified Health Plans Part I (CMS-9989-F) promulgated by HHS, clearly state that DPC is not health insurance, and that the law has its roots in a provision in WA state law (48.150RCW) defining DPC as a health benefit outside insurance. IRS Continues to give guidance that DPC plans are considered health plans under Sec. 223 (c) of the Internal Revenue Code (IRC), which prohibits HSA account holders with high deductible health plans from having a second “health plan.” DPC members have met with officials in the Department of the Treasury and continue to work with the administration and Congress to change the IRS definition so that DPC fees are qualified medical expenses under Sec. 213 (d) of the IRC and can be offered as a benefit complimenting Health Savings Accounts (HSAs) paired with high deductible health plans.
2014: Second National Gathering Focused On DPC (DPC) Held In Wash., DC. June 2014.
2014: DPC United, a new DPC Physician Association, launched by Dr. Samir Qamar of MedLion announces that it will provide resources for DPC physicians and consumers.
2014: Michigan DPC Bill Introduced as Louisiana Passes Law: On September 9, 2014, Michigan State Senator Patrick Colbeck (R-Canton) introduced S.B. 1033, a bill to amend the MI state insurance code to clarify that a DPC agreement is not subject to state insurance regulation. DPCC has provided resourced to Sen. Colbeck, and we are watching developments in state legislatures around the country as they prepare for the coming sessions. This summer, Gov. Bobby Jindal (R-LA) signed similar legislation; Senate Bill No. 516, making Louisiana the latest state to create law to define DPC practices correctly outside the scope of insurance regulation. Stay tuned for further updates as the legislative sessions kick off in this coming January.
2014: DPCC member Iora health recently announced an exciting new partnership with Humana to treat Medicare Advantage patients in Washington and Arizona. According to the Iora release, “The partnership launches Iora’s unique health care model in Arizona and Washington where Iora Health will open four new primary care practices – two in Phoenix and two in Seattle – under the Iora Primary Care brand. The primary care practices are designed exclusively for Humana’s Medicare Advantage members and will provide members access to affordable, quality care.”
2014: New Study Conducted by Optum and MDVIP Finds Personalized Preventive Care Significantly Reduces Healthcare Expenditures Among Medicare Advantage Beneficiaries
2014: September 2014, American Academy of Private Physicians (AAPP) Course Corrects Physician Association, citing that the industry’s association is focusing on five key areas. Those include: legal compliance for doctors, innovative learning tracks at national meetings, physician networking, legislative and lobbying initiatives and staying up to date on new and emerging technologies...
Your ability to withstand the pressure and overcome the obstacles of uncertainty
and potential failure and see the other side before others do is what makes a successful concierge [direct-pay] physician
“There are no insurance codes for ‘cure,’” says Dr. Garrison Bliss of Qliance, based in Seattle, WA.
2014: In October 2014, at the AAFP Assembly, a DPC Track is added to the agenda in Washington, D.C. It was called the “Health is Primary” initiative, a key business model for success touted by the AAFP (American Academy of Family Physicians).
2014: MD² Expands, Granting Access to Two New World-Class Medical Institutions; November 2014
2014: Washington State OIC issued DPC Outlook in Washington State. The OIC report insinuated that DPC is losing ground in terms of patients and that our monthly fees have been climbing (presumably as we head toward concierge medicine pricing).
2014: In reply, The DPC Journal assimilated a DPC leadership response to the Washington State OIC Report publishing for legislators, payers, physicians and the like: ‘DPC Leadership Response To Washington State OIC Report: ‘Outlook for DPC is bright throughout U.S.’
2014: The DPC Journal releases its industry-wide definition of DPC, the 5-Minute Guide: What Makes DPC Different From Concierge Medicine. Also releases 2-Year analysis of DPC marketplace data.
2014: (November 4, 2014) Hospitals Take Cues From The Hospitality Industry | By Kaiser Health News
2015: Michigan State Sen. Pat Colbeck, R-Canton, believes the path to providing Michigan citizens with access to higher quality, lower cost health care has been cleared following Gov. Rick Snyder’s signature into law of Colbeck’ s SB 1033 (Public Act 522 of 2014). The new law in Michigan assures physicians who adopt a direct primary care service business model that the administrative burden associated with insurance regulations will not interfere with their treatment of patients. Physicians who offer direct primary care services provide specified services for a monthly subscription fee that usually vary between $50 and $125 per month.
States with DPC Laws: Source: DPCare.org; Current as of January 22, 2015: Washington – 48-150 RCW; Utah – UT 31A-4-106.5; Oregon – ORS 735.500; West Virginia- WV-16-2J-1; Arizona – S.B. 1404; Louisiana – S.B. 516; Michigan – S.B. 1033
2015: Specialdocs, a pioneer and leading Concierge Medicine consulting firm says ‘Cardiology, Endocrinology, Pulmonology, Pediatrics and OB GYN Practices Can Benefit from Conversion to Concierge Model.’
2015: The United Hospital Fund Releases A Report, Convenient Care: Retail Clinics and Urgent Care Centers In New York State.
This report is relevant to Concierge Care and the DPC healthcare space because: Although based on a small sample from a single group practice in Minnesota, the study found that patients who visited retail clinics had lower total costs than matched patients who visited the acute care clinic (Rohrer, Angstman, and Bartel 2009). A more recent study of adult primary care patients, also in Minnesota, found that the odds of return visits for treatment of sinusitis were the same whether patients received care at a retail clinic or in a regular office visit (Rohrer, Angstman, and Garrison 2012).
Perhaps more telling, a larger study of spending patterns of CVS Caremark employees found a significantly lower total cost of care in the year following a first visit to a retail clinic compared to costs incurred by propensity score-matched individuals who received care in other settings. In total, retail clinic users spent $262 less than their counterparts, with savings stemming primarily from lower medical expenses at physicians’ offices ($77 savings) and reduced spending for hospital inpatient care ($121 savings). Retail clinic users also had 12 percent fewer emergency department visits than their counterparts (Sussman et al. 2013). The UHF saw nothing analogous on the impact of urgent care centers on total costs, but one study found that initial use of an urgent care center significantly reduced emergency department visits without increasing patient hospitalizations (Merritt, Naamon, and Morris 2000). Those results should be cautiously interpreted, however, given the study’s design limitations.
Conversely, in September 2014, the MDVIP model also was shown to have saved some $3.7 million in reduced medical utilization for the 2,300 MDVIP Medicare Advantage patients over two years. Savings were $86.68 per patient per month in year one, and $47.03 per patient per month in year two, compared with patients who did not join an MDVIP practice. The two-year study explored preventive healthcare’s ability to improve outcomes by creating a closer, personalized physician-patient relationship and focusing on disease prevention for Medicare Advantage.
2015: PinnacleCare, a leading health advisory firm, studied the impact of an expert second opinion on medical outcomes.
Researchers collected data on 1,000 cases over a three‐year period and found that almost 77 percent of medical interventions led to changes in diagnosis, treatment, and/or treating physician. PinnacleCare gathered data on patient outcomes from their interventions over a three‐year period. In a sampling of 1,000 cases with known outcomes from 2012‐2014, 41% resulted in transfer of care to a COE or expert provider with 34% resulting in a change in diagnosis, treatment, and/or course of care. A total of 18 patients were able to avoid unnecessary surgery as a result of a PinnacleCare intervention.
The data demonstrates the potential for health advisory services and second opinions to optimize outcomes and avoid needless expense. One of the persistent challenges in health care today is access to expert physicians. With consumer directed health care plans, the value of health advisory services becomes even more evident as consumers struggle with vetting appropriate providers and treatment options for their complex conditions while seeking timely access to the care that they need. PinnacleCare is committed to providing objective, concierge‐ level support with the expert resources and access needed to help consumers tackle these complex challenges.
2015: The DPC Journal to release its 2015 Annual Report and Market Trends Analyses In The First Quarter of 2015
2015: The DPC Journal releases physician insight gathered in a 2015 Industry Guidelines Proposal To Insurers and Legislators, Second Quarter 2015
2015: (December 2015) In 2015, fewer than half of the direct practices chose to report voluntary information. Some said they do not collect this information, and others simply did not respond to the supplementary questions. The bill requires the Office of the Insurance Commissioner (OIC) to report annually to the Legislature on direct health care practices. Under RCW 48.150.100(3), this includes but is not limited to “participation trends, complaints received, voluntary data reported by the direct practices and any necessary modifications to this chapter.”
2016: (October 2016) National trade publication, Concierge Medicine Today issues industry-wide “Position Statement” on Outdated Physician Referral Methods to Surgeons and Hospitals on Behalf of Patients.
2017: (January 2017) Las Vegas’ Turntable Health Closes | Jan. 2017 | ~Las Vegas Weekly | Leslie Ventura | Wed, Jan 11, 2017 (4:33 p.m.) Turntable Health, a membership-based primary care practice in Downtown Las Vegas, will close its doors on January 31. Touted as an affordable and comprehensive alternative to insurance-based healthcare, the Downtown Project-affiliated company notified its members in December that its services would no longer be available. The member-based model, in which patients pay a flat monthly rate of $80 to receive access to a “wellness ecosystem,” including same- or next-day visits; 24/7 physician contact by phone, email or video chat; health coaching; nutrition, yoga and group therapy classes; and an on-site demonstration kitchen. Read Full Story … Source: https://lasvegasweekly.com/intersection/2017/jan/11/turntable-healths-closure-leaves-downtown-patients/
2017: (May 2017) UnitedHealth shutting down Harken Health May 16, 2017 – Harken Health was never a major player in the insurance market, but its demise ends an experiment that company officials believed would reduce healthcare costs. The company lost nearly $70 million during the first six months of 2016 and never recovered. The closure will be disappointing for those promoting alternative care models as ways to improve outcomes while reducing costs and perhaps increasing patient’s satisfaction. In April 2016, then CEO Tom Vanderheyden told Healthcare Dive the company’s care teams would be “empowered with the time to listen and build authentic and trusting relationship with members.” ~HealthcareDIVE Insight | Les Masterson | May 16, 2017 Read More … http://www.healthcaredive.com/news/harken-health-closes-after-a-year-of-cuts-losses/442849/
2017: (May 2017) The DPC Journal has received multiple confirmations from various sources today [May 17, 2017] that reports from the Puget Sound Business (PBSJ) dated May 16, 2017 are confirmed … Qliance is closing their doors effective June 15, 2017. GeekWire reported today (May 17, 2017 @ 9:46 am) that … In an internal memo from Dr. Erika Bliss obtained by the PSBJ, she said the company was unable to find the funding to last them until they were able to find new contracts. The DPC Journal has confirmed this news as well.
2017: (August 2017) AAPP Board of Directors Votes to Suspend Operations and to evaluate AAPP’s value proposition for 2018 and beyond. They issued the following statements … Article/Story Written By Michael Tetreault, Editor
AUGUST 10, 2017 In a statement released to Concierge Medicine Today by Dr. Pamila Brar, current President of the American Academy of Private Physicians (AAPP) stated “Due to evolving marketplace conditions in the private medicine conference space, our AAPP board of directors voted to suspend operations in 2017 and to evaluate AAPP’s ongoing usefulness and value proposition for 2018 and beyond.”
Formerly known as the Society of Innovative Medical Practice Design (SIMPD) for many years, the AAPP’s presence, conferences and representatives served a limited, but engaged physician audience in unique ways. They focused on five key areas which included: legal compliance for doctors; innovative learning tracks at national meetings; physician networking; legislative and lobbying initiatives and staying up to date on new and emerging technologies. Although AAPP is suspending operations and evaluating the organization’s future, other physician organizations involved in private direct medicine seem to be experiencing strong membership growth.
Throughout an entire career however, physicians are faced with recurring questions related to medical associations: Which associations should I join? Which should I retain membership in? How do you decide which associations to pass on altogether? Simply type in the words ‘medical association’ and 29,200,000 plus results are found on Google alone.
A recent story in Forbes noted that ‘Nonprofits can be a great way for a community to mobilize around a cause, make an impact and deliver services to those in need.’
Following that, in November 2016, Becker’s Hospital Review cited relevant physician association challenges and wrote that nationally, 57.4 percent of physicians are part of a state medical society; 73.8 percent of physicians are members of a national specialty society; 31 percent of physicians are a current Member of the American Medical Association; and finally, 10.1. percent of physicians are a Member of the American Osteopathic Association. [1]
However, even with so many options today and increasing annual dues, the membership of the American College of Physicians nearly doubled between 1995 and 2009, reaching 130,000 members. The American College of Surgeons, with 77,000 members, has also seen tremendous growth in the past three decades. In June, the American Academy of Family Physicians announced that its membership had reached an all-time high of 100,300. [2]
So what makes these groups different from others?
Most doctors join medical societies and associations for what they can get, not for what they can contribute. Maybe this paradigm should be reversed, like many antiquated processes in today’s healthcare marketplace. Often the decision to join is influenced by a medical association’s position on hot-button political issues, such as healthcare reform. Many medical associations’ benefits are similar: access to discounts on medical devices; discounts on malpractice insurance; CME credit courses and webinars; hands-on help in choosing an EMR/EHR; participation at national or regional events and conferences; and advocacy for issues affecting members. It’s the last benefit where the difference in associations is generally revealed.
Optimism regarding Concierge Medicine, the delivery of Direct Primary Care and other private medicine business structures remains high among both consumers, executive healthcare professionals and physicians alike. In fact, a recent career satisfaction poll of the private physician community [e.g. Concierge Medicine, Direct Primary Care, Micro Clinic, etc.], reveals that nearly 90% of physicians in this niche community of healthcare professionals are highly satisfied with their career move into these entrepreneurial healthcare delivery business models There are models in which patients pay either an annual membership or monthly fee to be a part of the doctor’s practice.
“I think that this is an exciting time for private direct medicine,” says attorney Jim Eischen, Esq. “With all sorts of stakeholders exploring private medicine solutions: this is no longer primarily a solo or small physician-owned medical practice space. Larger systems and providers, and even non-provider enterprises, are all exploring how to accomplish improved health outcomes with private consumer investment and expanded communication/connection. But there are challenges with how to integrate with the tax code, and with plan requirements.”
However, the trend lines in Direct Primary Care (DPC) for example, reveal that the independent, solo physician is regrouping and possibly consolidating in its service line offering after two DPC groups announced their closures earlier this year [2017]. When asked, ‘Will DPC Stay Small? Grow Big? Optimism? What’s in store for Direct Primary Care?’ more than 13% of physicians are hopeful HSA and FSA integration inside DPC will occur to help patients pay for their monthly memberships. Additionally, nearly 18% of respondents to the online poll stated ‘I hope DPC Doctors Can Work/Partner With More Businesses to Save HC Costs …’ and nine percent noted ‘I hope to see the creation of DPC networks for Employer Use (sim. to MCOs) come into the market.’ Self-insured employers are beginning to show interest in the ways in which these models can improve health outcomes and contain costs according to several industry insiders.
“There is no better strategy than a major issue campaign to increase the number of people in an association or professional society,” said the Publisher of Concierge Medicine Today, The Direct Primary Care Journal and Concierge Medicine Today. “If properly managed, associations will use a new issuecampaign as an opportunity to expand their sources of information and the number of people involved in that aspect of the work. Most organizations focus on building a membership network and often underestimate the need to build the value of their own organizations while struggling to win on public issues. As in the case of the corn farmer from Iowa, the thought is ‘if you build it, they will come.’”
When nearly sixty percent of physicians in 2017 cite that they took Less than 5 Business Education courses …, certainly associations and physician groups must adapt to the needs of its base. However, Concierge Medicine and its variants operating in the U.S. today work because so many people have made it work. Concierge Medicine and the like, work because a few visioneering physicians broke every standard delivery tradition they knew to embrace the mission of the Golden Rule: Treat others the way you would want to be treated.
“Since AAPP was originally designed to help support self-employed physicians seeking to convert to a private direct model, I think demand for live conferences focused on self-employed physicians limits the draw,” says Eischen. “More web-based education, along with live conferences structured to integrate the entire range of stakeholders, is the probable downstream solution for moving private direct medicine conferences/education forward.”
“Comprehensive Pharmacogenomics for example, is a powerful healthcare innovation,” adds CMT Publisher. “Concierge Medicine is seen by many as providing the ideal delivery model for the future of precision medicine. Used under the guidance and application of a Concierge Physician, these innovative tests can have a predictive effect on patient treatment outcomes. Whole genome sequencing, genetic testing and comprehensive profiling with more than 50 well-established pharmacogenomics genes in a single, cost-effective test can provide medically actionable and clinically relevant data, allowing Concierge Physicians, to make a more informed and thoughtful treatment recommendation for the health and well-being of each patient. Concierge Medicine Today strongly supports use of this innovative testing.”
“Future growth of private direct medicine may not look like the past,” concludes Eischen. “As a more diverse array of stakeholders need to come together to balance how to better integrate private health and wellness services with the traditional diagnosis and treatment services of plan-reimbursed healthcare.”
[1] – http://www.beckershospitalreview.com/hospital-physician-relationships/112-statistics-on-physicians-under-45-years-old-practice-setting-finances-future-plans-more.html; 112 statistics on physicians under 45 years old — practice setting, finances, future plans & more Written by Laura Dyrda; November 02, 2016
2017: (August 10, 2017) In a statement released by The Direct Primary Care Journal, the trend lines in 2017 related to Direct Primary Care (DPC) for example, reveal that the independent, solo physician is regrouping and possibly consolidating in its service line offering after two DPC groups announced their closures earlier this year [2017]. When asked, 'Will DPC Stay Small? Grow Big? Optimism? What's in store for Direct Primary Care?’ more than 13% of physicians are hopeful HSA and FSA integration inside DPC will occur to help patients pay for their monthly memberships. Additionally, nearly 18% of respondents to the online poll stated 'I hope DPC Doctors Can Work/Partner With More Businesses to Save HC Costs ...' and nine percent noted 'I hope to see the creation of DPC networks for Employer Use (sim. to MCOs) come into the market.' Self-insured employers are beginning to show interest in the ways in which these models can improve health outcomes and contain costs according to several industry insiders.
2017: (August 2017) OCTOBER 27-28. 2017 | ATLANTA, GA USA | Concierge Medicine Forum in Atlanta to Showcase “Precision Medicine” Use, Utility and Innovation
2018: (January 2018) CMT, PHYSICIAN POLL, 2018: Does your Concierge Medicine Practice bill Medicare?
2018: (April 2018) CMT SURVEY SAYS … 1K+ PATIENTS SAY … “The Patient Experience Matters to GUESS WHO, THE PATIENT — and So Does Air Quality In Your Primary Care & Family Care Practice.”
2018: (June 1, 2018) Press Release, RANKED: Top 20 Web Sites In Concierge Medicine Revealed by Concierge Medicine Today, LLC. — 2018-2019
2018: (June 25, 2018) Press Release, ACEP, PHYSICIAN GROUPS: PRICE TRANSPARENCY MUST INCLUDE HEALTH INSURERS
2018: (June 27, 2018) New Study, MDVIP: The Grades Are In; Most Americans Score an ‘F’ on Fat IQ Test
2018: (Oct. 26-28, 2018) Concierge Medicine Today hosted the 2018 Concierge Medicine Forum in Atlanta, GA USA
2019: National Study Finds Americans Don’t Know the Facts or Their Risk for Heart Disease; Jan 2019
2019: (March 6, 2019) Dr. Garrison Bliss writes a blog story entitled The Origin of DPC:Transformation, Simple Ideas, and Trojan Horses; Moving into Subscription medicine -- Two of my partners from my original practice eventually left to set up MD2, the first monthly fee practice in the US. At $1000 per member per month, MD2 was also the first ridiculously priced primary care practice, so it attracted comments in the press about concierge care and boutique primary care. When I looked at financing an optimized primary care system, I was attracted to the monthly fee concept. Primary care is a fixed-cost business, so a monthly fee could replace the fee-for-service insurance model, with its foolish incentives and toxic costs. I calculated the lowest monthly fee that could support a 600-800 patient panel at $30-50 per patient per month (depending upon age). It worked both as a care model and business model, so Mitch Karton and I launched the new Seattle Medical Associates in 1997, filling our practices in just over a year. Roughly 3 years later, I moved on to supporting a national movement through a board position in the American Society of Concierge Physicians, started by Dr. John Blanchard, which later became the Society for Innovative Medical Practice Design, and eventually the American Academy of Private Physicians.
2019: The X Factor: for Women, the Rewards of Concierge Medicine are Even Greater, According to Specialdocs; Aug 2019
2019: MDVIP Reaches Major Milestone of Over 1,000 Primary Care Physicians Nationwide; Oct 2019
2019: (Oct. 24-26, 2019) Concierge Medicine Today hosts the industry's annual conference, the 2019 Concierge Medicine Forum in Atlanta, GA USA
2020: Paragon And SignatureMD Merge To Establish Premier Provider Of Membership-Based Concierge Medicine Support Services; April 2020
2020: OFFICIAL, POSITION STATEMENT | Concierge Medicine Industry Leadership Share Their Opinions On the Critical Protocols and Best Practices Related to Resourcing and Distribution of COVID-19 Vaccine; April/May 2020
2020: MDVIP Membership Medicine Model Significantly Cuts Diabetes Care Costs; June 2020
2020: In the Wake of COVID-19, Specialdocs Reports Rapid Growth in Its Network of Independent Concierge Physician Practices; June 2020
2020: Pandemic is Disrupting Healthcare Routines, Challenging Psyche of Americans Across Generations, Reveals New Study from MDVIP and Ipsos; Aug 2020
2020: Study Finds Many Americans in the Dark About Dementia And Alzheimer’s Disease, Uncovers How Pandemic Is Affecting Brain Health; Sept. 2020
2020: (Nov 2020) Concierge Medicine Today hosts the industry's first virtual conference due to the pandemic, the 2020Concierge Medicine Forum in Atlanta, GA USA
2020: Specialdocs Informs and Inspires at Concierge Medicine Industry's Signature Event Nov. 12th - 14th
2021: Survey shows zero percent pandemic closure rate for membership-based medical practices; March 12, 2021; Dr. Dean McElwain; Dean McElwain is co-founder, president & CEO of Castle Connolly Private Health Partners.
2021: MDVIP Named to Fortune 2021 Best Workplaces in Healthcare & Biopharma™; March 2021
2021: SignatureMD Completes Merger with Cypress Membership Medicine; March 31, 2021
2021: MDVIP Primary Care Model Reduces Incidence Of Cardiovascular Events In At-Risk Patients; April 2021
2021: New Study Finds Alarming Gaps in Women’s Health Knowledge and Healthcare Experiences; May 2021
2021: Concierge Medicine Pioneer Specialdocs Launches First Women Physicians Council; Aug 2021
2021: Goldman Sachs Asset Management and Charlesbank Capital Partners Complete Acquisition of MDVIP Primary Care Network; Oct 2021
2021: (Oct. 21-23, 2021) Concierge Medicine Today hosts the industry's annual conference, the 2021 Concierge Medicine Forum in Atlanta, GA USA
September 2022: CCPHP’s CEO Dean McElwain named Most Influential CEO of 2022 – New York
August 2023: (MDVIP; Press Release) Inflammation Marker Signifies Increased Mortality Risk, Finds New Study in PLOS ONE
September 2023: MDVIP Ranked Among Fortune’s Best Workplaces in Healthcare™ for Third Consecutive Year
October 2023: Concierge Medicine Today hosts “sold out” Physician education conference in Atlanta, GA USA for Physicians within the industry and those wanting to learn more.
January 2024: Concierge Medicine is Set to Soar in 2024 [Specialdocs]; Specialdocs Reports a Robust 2023 as 21 New Healthcare
Did We Miss Something? It wasn’t on purpose! Do We Need To Add Something? Please let us know. Contact us here.
Editor's Note: This is by no means an all-inclusive, every single detail about all of the things that have occurred in this unique healthcare delivery space. It is a summary of many of the highlights however. When possible, we've tried to provide links to the stories, web sites, press releases, research, studies and organizations for you to learn more. We recognize a lot has happened in the past 20+ years. And, it’s virtually impossible to capture every moment in one document or on one page. As you may be aware, this document is routinely updated by Concierge Medicine Today, LLC., and is routinely edited, corrected and updated. If we missed something or you think we should add something, please, let us know by emailing us directly at editor@ConciergeMedicineToday.com. Thank you!
Why would concierge medicine work for you? 4 questions to consider.
It all begins with an idea.
If you're thinking about starting a concierge medicine practice it is important to answer the question, why is this going to work? Maybe you've been circling the air space around concierge medicine or a similar subscription-based healthcare delivery program offering for a while now. Perhaps you're ready to take the next stop of contacting a consulting firm. That's amazing! Well done.
However, before you take the leap you may want to do a little homework and get a baseline.
Oxford Languages describes a baseline as a minimum or starting point used for comparisons.
For nearly two decades, we've observed that part of being successful as a concierge medicine practice is having a uniquely better patient experience.
But, you and I both know that unique isn’t enough. You can be uniquely bad.
Why are you smirking? ;)
Unique doesn’t create that positive word of mouth patient story that's going to be repeatedly shared among the Mom-group at the bus stop.
Most medical practice patient experiences we've all encountered let's be downright honest here ... are dull, laborious and anything but unique.
Recently we spoke to a dentist who was helping his wife, a Physician, start her own concierge medicine practice. A couple of months after she started, her husband (the Dentist) called us up and said "Michael, you were right! It is so easy to impress patients. It's so bad out there we don't even have to do much ..."
He's absolutely right.
You don't have to do much.
How do I know? Well, I'm not a Physician but I am a Patient so I know exactly what it's like to sit on the other side of the exam room. Worse yet, the waiting room.
If it sounds like we're being harsh it's only because I care. I care about what my Doctor says. I care about his/her words they speak into my health and life. After all, five words from my Doctor carry more weight than fifty words about 'em.
Unfortunately, in healthcare today there are a lot shared assumptions that cause us all to do the same things, the same way.
We spoke not too long ago with a medical professor who worked at some very well-known medical schools. She said '…not only is it going to take an act of Congress to change how and what we teach [Doctors] in medical school ... it will take an act of God.'
I think she's right.
But, that shouldn't deter or derail you or I from our mission and purpose of leaving healthcare better than it found us.
Hmm. That begs the question, is a uniquely better patient experience a solution to a problem you might be trying to solve, especially when it comes to your reluctance possibly to finally start or enter concierge medicine?
Greystone Global recently wrote ... Uniquely better will come along for every industry. Because somebody, somewhere, is messing with the prevailing model. The question is, will you (and your organization) be positioned to recognize it? Here are a few examples that come to mind that could be organizations who were positioned to recognize uniquely better. Is Starbucks coffee uniquely better? Are Apple products uniquely better? Is Amazon a uniquely better way of shopping? Is Uber uniquely better than a taxi? Is an ice bucket challenge a uniquely better way to fundraise? Is your culture ready to recognize uniquely better, or will it pass you by and will your organization be left behind?
Tomorrow, more practices, more programs and more Physicians' will learn that their job each day is to create a culture of gratitude for their Patients. They'll create uniquely better patient experiences by incorporating customer service training strategies into every staff-patient tension point. The world outside of healthcare spends millions of dollars and thousands of hours each year training teams and individuals on customer service tactics. Concierge medicine knows this and is doing the same in a lot of practices out there. Hospitals, retail healthcare clinics, telehealth companies, executive healthcare programs and even specialty medicine practices are learning from what concierge medicine is doing and taking notes about the uniquely better patient experiences these doctors, practices and programs have and continue to curate.
I'll leave you with the four questions one speaker left the audience with not long ago at a conference called the Leadership Summit. And no, this wasn't a healthcare conference. But oddly enough, we think the answers you may find if you just take the time to ask them ... could change your practice [and healthcare] for the better!
Is this unique?
What would make it unique?
Is it better?
Is it better…really?
Originally Written Sept 2023 by Editor, Concierge Medicine Today